


Abstract
Background: Given the limitations of available literature, recommended time targets for cancer treatment are based on expert opinion. In this study, we investigated the association of time to surgery and important clinical outcomes in patients who underwent surgery for primary rectosigmoid cancer.
Methods: We conducted a retrospective cohort study of patients who underwent nonemergent curative-intent resection for rectosigmoid cancer at a tertiary academic hospital system between January 2002 and June 2018. We fit multivariable regression models using restricted cubic splines to assess for a nonlinear association of time to surgery with overall survival, disease-free survival and major 30-day postoperative complications.
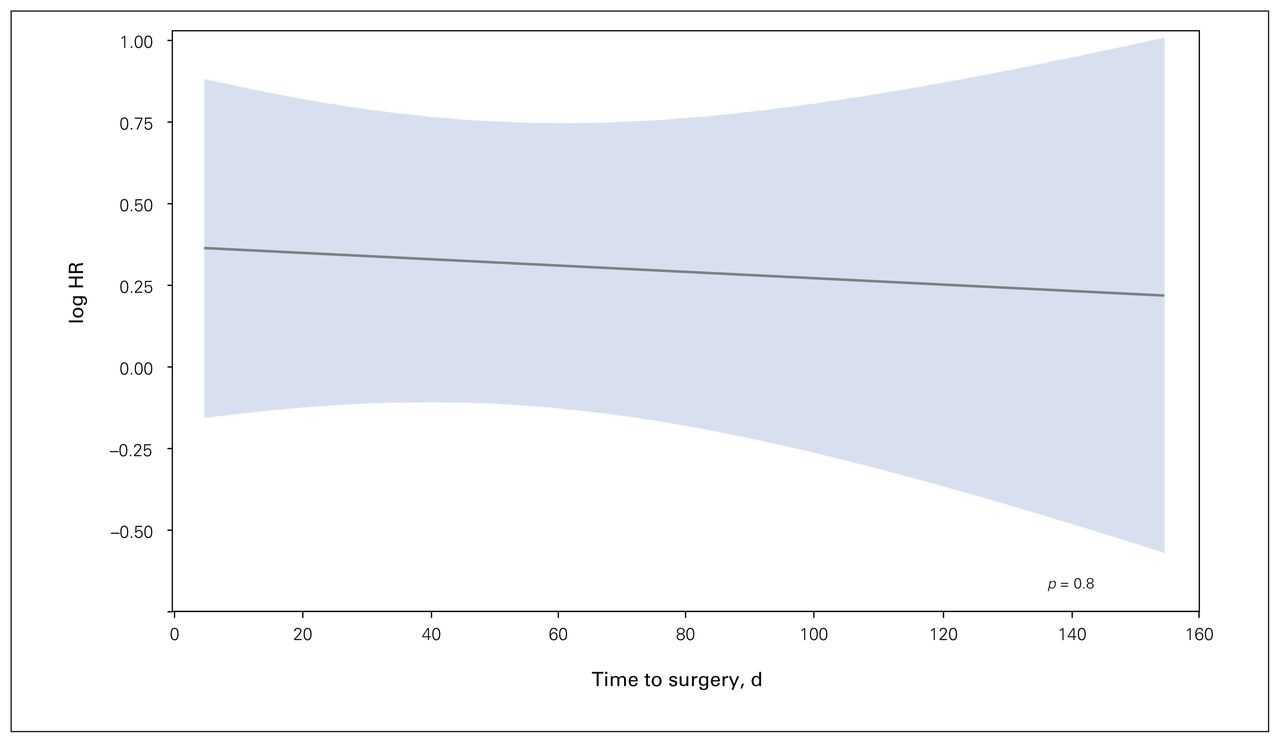
Results: A total of 714 patients met the inclusion criteria. The median time to surgery was 49 days. A nonlinear association of time to surgery was not observed with overall survival (nonlinearity p = 0.09), disease-free survival (nonlinearity p = 0.06) or major complications at 30 days (nonlinearity p = 0.8). Secondary analysis excluding patients who underwent neoadjuvant therapy showed no association between time to surgery and survival (p = 0.2). Analyses when assessing for linear associations and when dichotomizing time to surgery into early (< 60 d) and late (≥ 60 d) groups showed no association with overall survival.
Conclusion: In a tertiary cancer centre where clinical triaging is possible, there was no association of time to surgery with oncologic surgical outcomes in patients treated for primary rectosigmoid cancer. Within specialized cancer centres in a universal health care model, at least for the time-to-surgery durations observed in our cohort, differences in time to surgery are unlikely to affect important clinical outcomes.
There is a perception that rapid initiation of cancer treatment improves outcomes.1–4 However, the relation between time to treatment and oncologic outcome varies by cancer type.5–7 In colorectal cancer, studies investigating the association of wait time with outcomes have given conflicting results.5,8–11 Contradictory results may be simply due to arbitrary categorization, ignoring the nonlinear continuous nature of the time-to-treatment variable.12–14 The practice of categorizing continuous variables carries the risk of inaccurate, misleading and possibly equivocal results.14–19
The unique complexity of surgical resection of low left-sided colorectal cancers compared to right-sided resections is well known. These patients often require more operative time, have increased postoperative morbidity and reoperation rates, have prolonged hospital length of stay and require more intensive preoperative investigations.20–22 Thus, decision-making pertaining to delays in time to treatment for rectosigmoid cancers may be uniquely affected, and investigation is paramount. For this reason, at a time when operating room use is limited and triage decision-making is critical owing to COVID-19-induced limitations, we sought to investigate the unique association of time to surgery with overall survival, disease-free survival and postoperative complications in patients undergoing surgery for primary rectosigmoid cancer, for cohorts including and excluding patients undergoing neoadjuvant treatment, within specialized cancer centres in a universal health care model. We treated time as a nonlinear continuous variable to avoid the pitfalls seen in previously published studies that treated time as a linear or categorical variable.5,8,11
Methods
This study was approved by the University Health Network Research Ethics Board and is reported in accordance with the RECORD statement.23
Study cohort and data sources
We identified all patients who underwent surgical resection for primary rectosigmoid cancer between January 2002 and June 2018 at a tertiary academic hospital system. We excluded patients who received emergency operations, those without 30-day follow-up data available, and those who did not have curative-intent surgery. Data were extracted from institutional prospectively maintained databases, the electronic medical record, the American College of Surgeons National Surgical Quality Improvement Program database (ACS NSQIP) and an internal cancer registry (eCancerCare).24 Two researchers (H.A.Q., A.D.) abstracted and collated data from these sources, with ongoing data quality checks.
Baseline covariates collected were age, sex, American Society of Anesthesiologists (ASA) classification and comorbidities. Tumour characteristics included stage from the 7th edition of the AJCC Cancer Staging Manual, TNM classification from surgical pathology reports and tumour location from operative reports. Tumour location was characterized as rectosigmoid (above the peritoneal reflection) or rectum (below the peritoneal reflection). Oncologic data included receipt and timing of chemotherapy and radiotherapy, dates of therapy commencement and completion, and surgical approach.
We defined time to surgery as the duration from diagnosis date to date of surgery. We identified the date of diagnosis as defined by the date of colonoscopy with confirmed pathologic diagnosis from the eCancerCare database, and date of surgery from the operative report in the electronic medical record. For patients who received neoadjuvant treatment, we identified dates of chemoradiotherapy initiation and completion, and, per institutional guidelines, added 8 weeks of planned delay to this to adequately quantify the complete neoadjuvant treatment period. For quantifying time to surgery for patients who received neoadjuvant treatment, we subtracted the neoadjuvant treatment and delay period.
Outcomes assessment
Outcomes of interest were overall survival, disease-free survival and rate of 30-day major postoperative complications. We defined overall survival as time from surgery to death from any cause, determined from the medical record and the eCancerCare registry. We defined disease-free survival as time from surgery to death from any cause, or cancer recurrence, using a standard surveillance regimen. We classified major postoperative complications within 30 days of surgery as Clavien–Dindo class III–V.25,26 We used the ACS NSQIP database to identify postoperative complications.
Statistical analysis
We summarized baseline patient characteristics, tumour characteristics and oncologic treatment data using descriptive statistics. We fit multivariable models to assess the association of time to surgery with each outcome. For our time-to-event outcomes of overall survival and disease-free survival, we fit multivariable Cox models, and for major complications, we fit multivariable logistic regression models, adjusted for age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy.27,28
We included time to surgery as a nonlinear continuous variable using restricted cubic splines to avoid making assumptions about the linearity of the relation of time to surgery with outcomes.12–14 For comparison with prior literature, we also fit a linear model of time to surgery with outcomes, as well as identified an inflection point in the function of time to surgery with outcomes to serve as a cut-point to dichotomize the time variable. Because neoadjuvant treatment and stage IV disease may alter clinical outcomes, we conducted 2 sensitivity analyses to exclude each set of patients.
We conducted the statistical analysis in R Studio (version 1.1.456, R Foundation for Statistical Computing). A 2-tailed p value < 0.05 was considered statistically significant.
Results
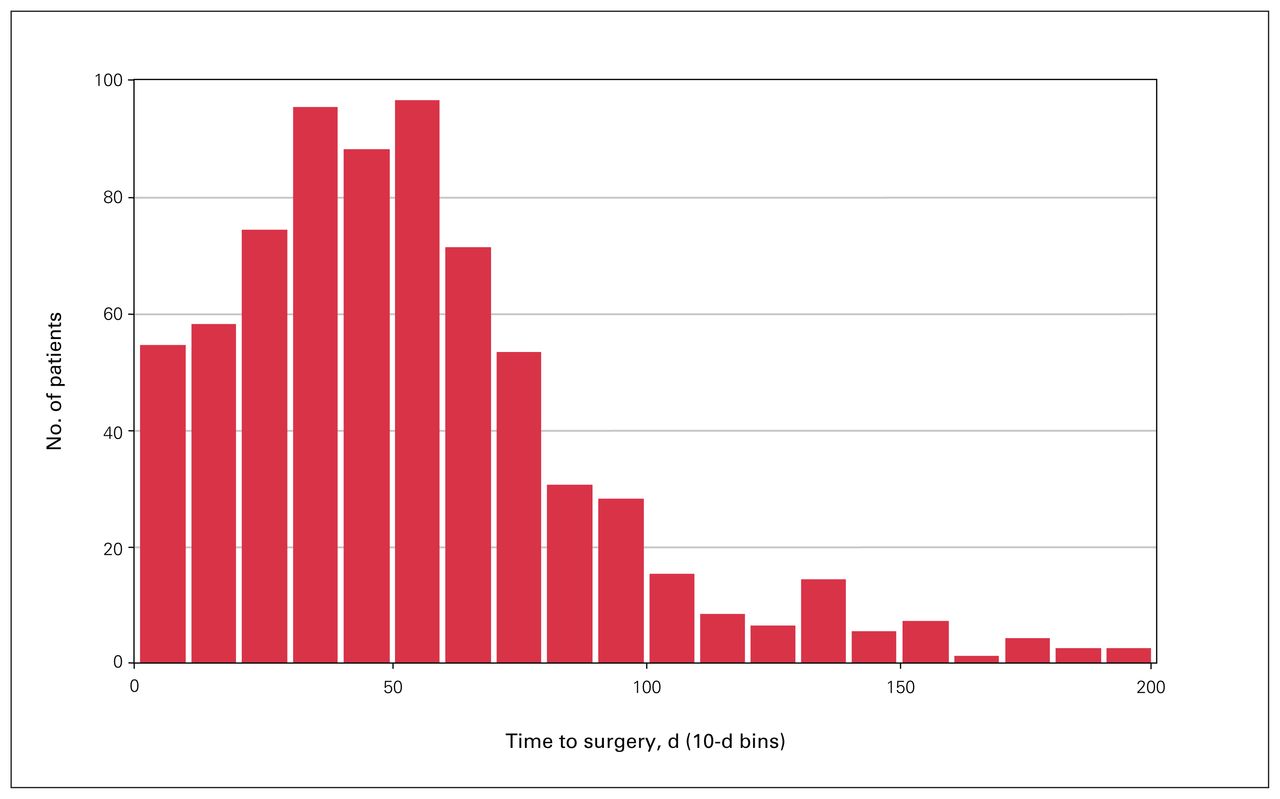
We identified 714 patients who underwent nonemergent oncologic resection with curative intent for primary rectosigmoid cancer (Figure 1). Outcome variables were available for all patients. Patient characteristics, tumour characteristics and oncologic treatments are shown in Table 1. Figure 2 shows the distribution of time to surgery. The median time to surgery was 49 (interquartile range [IQR] 29–70) days. Of the 714 patients, 215 (30.1%) had a complication, including 68 (9.5%) with major complications (Clavien–Dindo class III–V) in the 30 days after surgery. The median follow-up time for survival assessment was 60 (IQR 25–111) months. During this follow-up period, 120 patients (16.8%) had a recurrence, 216 (30.2%) died, and 259 (36.3%) had a recurrence or died.

Flow diagram showing study cohort selection.
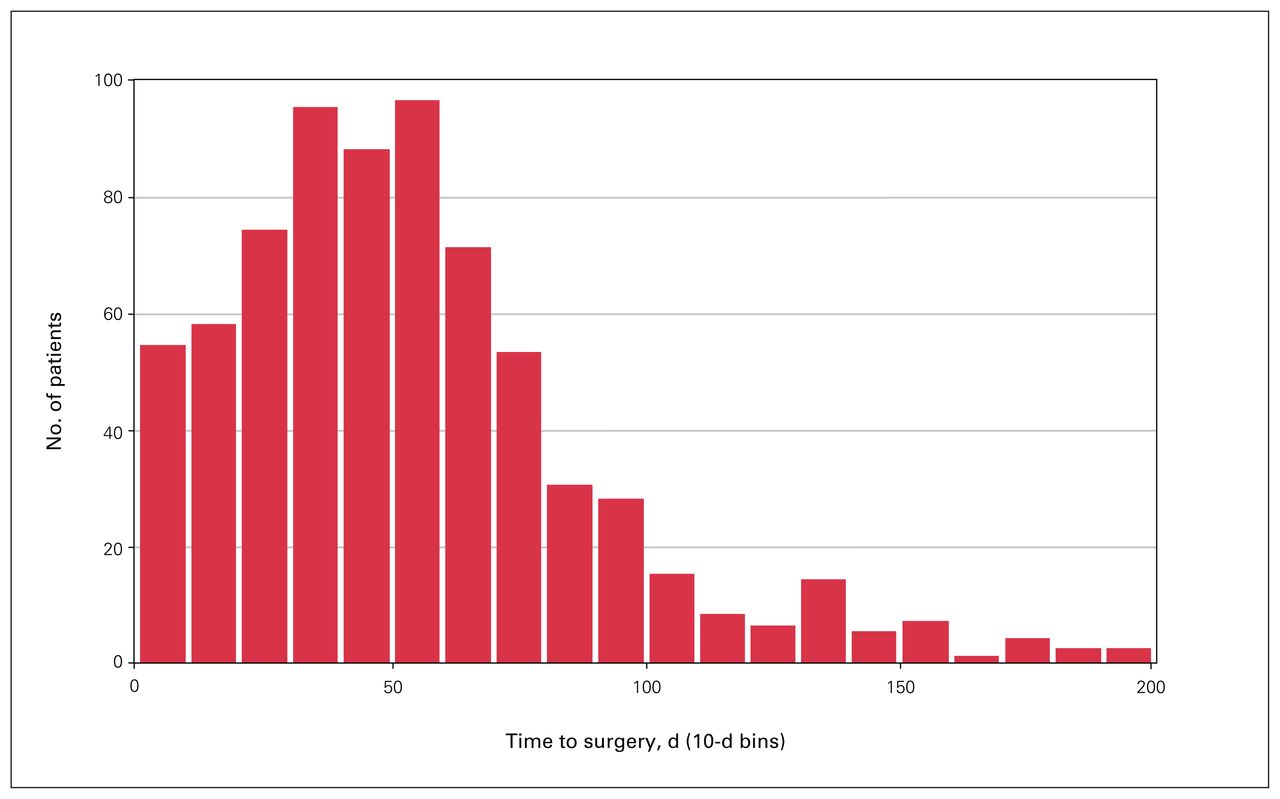
Histogram of time to surgery.
Baseline patient and tumour characteristics, and oncologic treatments
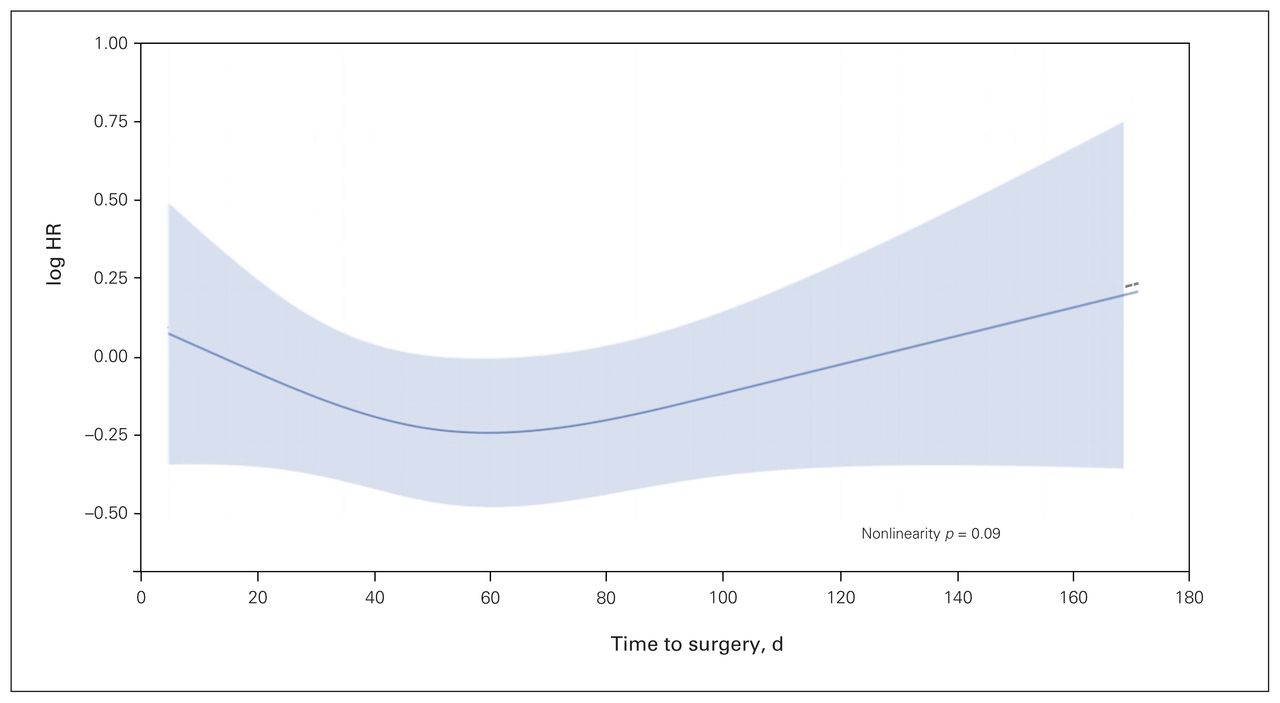
For overall survival, our first multivariable Cox model included time to surgery as a nonlinear continuous variable using restricted cubic splines adjusted for age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy. The relation of time to surgery with overall survival is shown in Figure 3. A nonlinear association of time to surgery and overall survival was not observed (p = 0.09). We conducted 2 sensitivity analyses excluding patients with stage IV cancer (n = 91) and those who underwent neoadjuvant therapy (n = 188), and the results also showed no nonlinear association between time to surgery and overall survival (p = 0.09 and 0.2, respectively). In our subsequent analyses using time as a linear variable and as a dichotomized variable, associations with overall survival were similarly not observed (Figure 4 and Figure 5). Restricted cubic splines model visually identified a nadir cut-point for time to surgery at 60 days, which was used for the dichotomized variable analysis (Figure 6).

Restricted cubic spline modelling of the relation between time to surgery and overall survival. The log of the hazard ratio (HR) derived from the multivariable Cox model including time using restricted cubic splines is shown on the y-axis versus time to surgery. The adjusted model includes age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy. Shaded area represents 95% confidence intervals of the adjusted HRs.

Linear modelling of the relation between time to surgery and overall survival. The log of the hazard ratio (HR) derived from the multivariable Cox model including time as a linear variable is shown on the y-axis versus time to surgery. The adjusted model includes age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy. Shaded area represents 95% confidence intervals of the adjusted HRs.
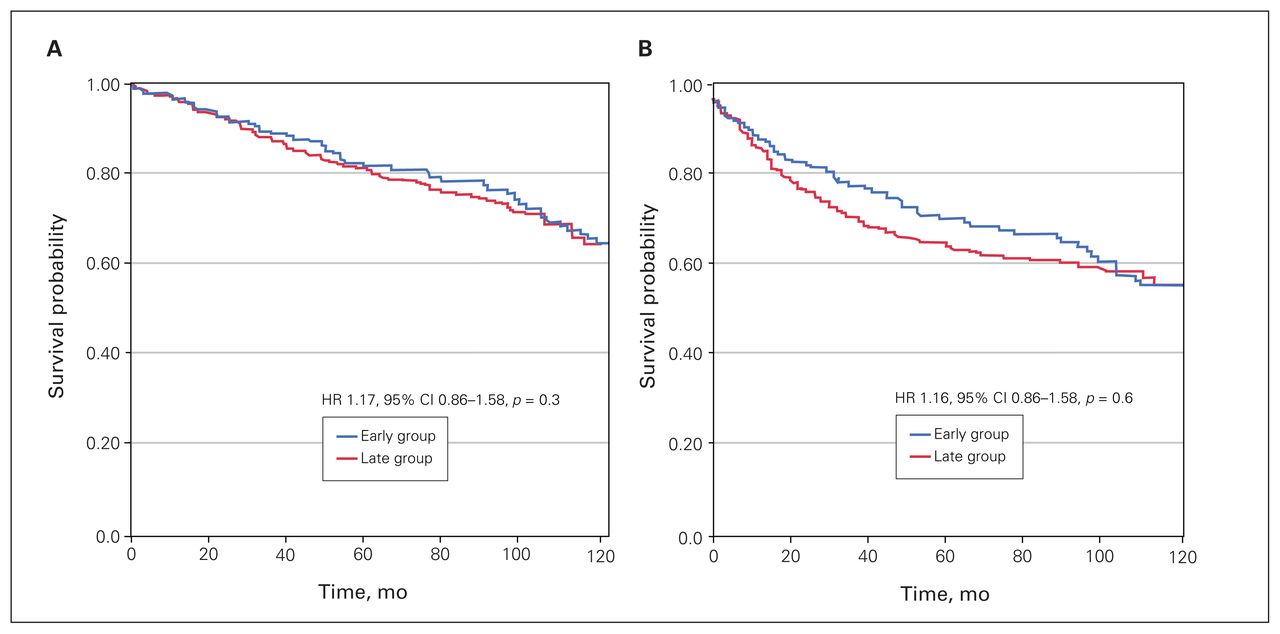
Overall (A) and disease-free (B) survival for the early (< 60 d) and late (≥ 60 d) time to surgery groups. The adjusted models included age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy. Adjusted hazard ratios (HRs) are shown.
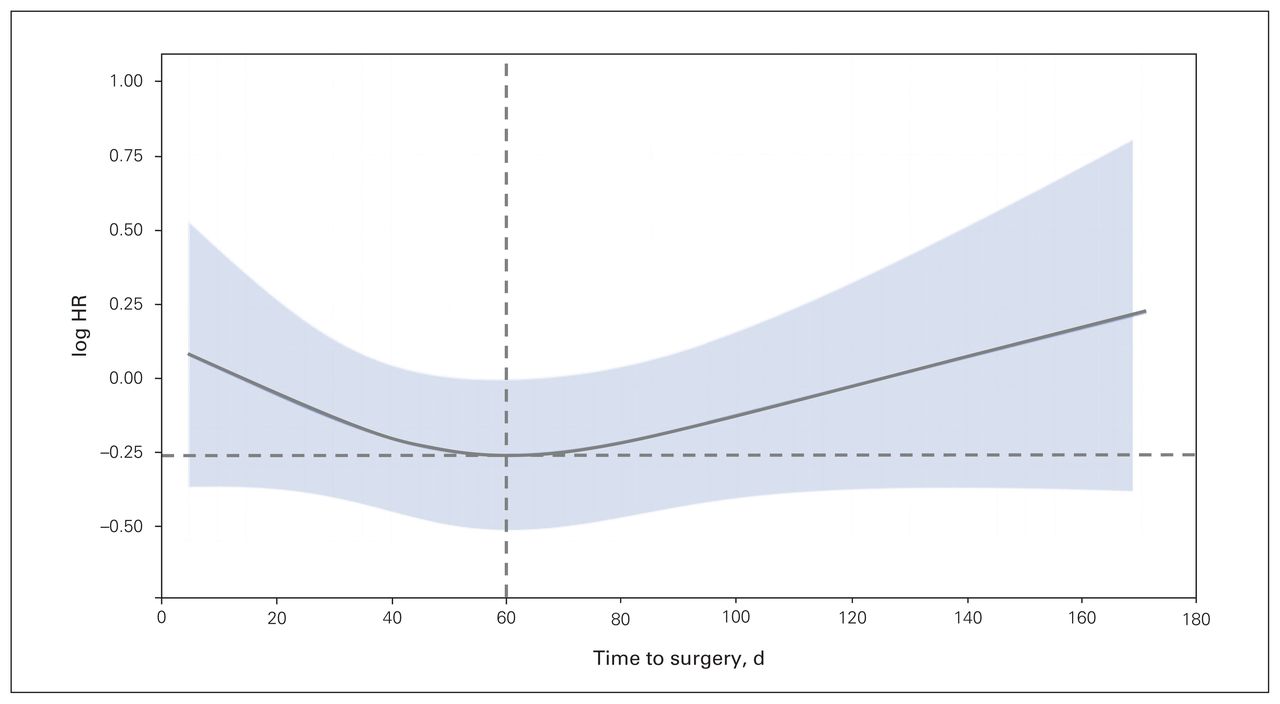
Restricted cubic spline modelling of the relation between time to surgery and overall survival visually identifying a cut-point. The log of the hazard ratio (HR) derived from the multivariable Cox model including time using restricted cubic splines is shown on the y-axis versus time to surgery. This was used to visually identify a nadir cut-point at 60 days (dotted lines). The adjusted model includes age, tumour site, comorbidities, stage, neoadjuvant therapy and adjuvant therapy. Shaded area represents 95% confidence intervals of the adjusted HRs.
The results were similar for disease-free survival and major complications. A nonlinear association of time to surgery and disease-free survival was not observed (nonlinear p = 0.06). Associations with disease-free survival and major complications were also not observed when time was treated as a linear or dichotomized variable.
Discussion
The importance of time to surgery is pressing in the setting of increasingly strained health care resources, especially in the context of a global pandemic. Accordingly, surgeons and health care administrators have been encouraged to find evidence to support challenging triage decision-making.29 In this study, associations of time to surgery with overall survival, disease-free survival or major complications were not observed in patients who underwent nonemergency curative-intent resection of primary rectosigmoid cancer at tertiary academic cancer centres in a universal health care model. This was true when time was appropriately treated as a nonlinear continuous variable to avoid arbitrary categorization and assumptions of linearity of the time variable. Our findings were also consistent in secondary analyses treating time as a linear and dichotomized variable, and when patients with stage IV disease and those who had had neoadjuvant therapy were excluded in sensitivity analyses. In specialized cancer centres within a universal health care model, differences in time to surgery are unlikely to affect important clinical outcomes, at least for the durations of time to surgery observed in our cohort, with a median of 49 days.
Although surgeons have been trained to appropriately triage and prioritize their patients, our findings can help to reassure surgeons and their patients that delays in surgery owing to system- or patient-dependent factors do not result in clinically significant changes in patient outcomes. We encourage physicians and surgeons, especially those in single-payer health care systems, to use these results to support evidence-based care plans for patients with rectosigmoid cancer and enable more appropriate resource allocation during times of crisis. It is important to acknowledge that curative-intent therapy for rectosigmoid cancer depends on the eventual delivery of surgical care. In addition, the present analysis excludes patients requiring emergency resection; thus, symptomatic presentation may warrant more urgent surgical management than suggested by our findings.
Prior studies that categorized time have shown associations of time to surgery with survival. In a prospective population-based Danish study, Iverson and colleagues8 selected a 60-day threshold for analysis and found poorer survival in patients with rectal cancer who waited 60 days or more than in those who waited less than 60 days; however, there was no such association in patients with colon cancer. Those authors selected the 60-day threshold based on results from a previous study identifying day 60 as a clinically significant cut-point.30 In a study from the United States, the authors arbitrarily separated time to surgery into 30-day intervals and identified optimal survival in patients who waited less than 30 days for their operation.11 Conversely, the authors of an Ontario-based population study used a guideline-recommended target for time to surgery of 42 days to dichotomize the time variable and observed no association with survival.10 An expedited 2-week diagnosis-to-treatment pathway was investigated in several single-institution retrospective studies: 2 studies showed no association of wait time with survival at 2 and 5 years, and 1 showed longer median survival with the 2-week pathway.9,31,32 Thus, treating time as a categorical variable has led to a wide range of results in both population-based and single-centre studies. Two studies of time to surgery in colon cancer treating time as a categorical variable and based on the US National Cancer Database showed increasing hazard of death with time to surgery greater than 40 days and 60 days, respectively.11,33 For many of these studies, discrepancies with our results may be due to the heterogeneity of colon cancer phenotypes in the patient cohorts, as well as varying methodologic use of the time-to-surgery variable.
Limitations
Limitations of our study include those inherent to all retrospective studies. To mitigate the risk of measurement bias, we used several independent, reliably abstracted databases.24 We used regression analysis to adjust for potential confounders, but adherence to neoadjuvant treatments, toxic effects from neoadjuvant treatment, preoperative functional impairment or frailty, and delays owing to personal or logistic reasons could not be included in the adjustment. Residual confounding due to unmeasured covariates may be present, but this is more likely to result in an overestimation of associations rather than a null effect. This cohort was sampled from a single tertiary care centre, and, given the relatively small sample and unique practice setting, these results may not be wholly generalizable to other settings. It is possible that other outcomes not assessed in this study, including patient-reported outcomes such as satisfaction, quality of life, symptom burden, fear, cancer-related distress and psychologic well-being, are associated with time to surgery; these ought to be investigated in future studies.
It was not known whether the association of time to surgery with outcomes would differ based on receipt of neoadjuvant treatment. We strived to address this concern through 2 modifications in our analysis: first, when calculating time to surgery for this patient population, we subtracted the neoadjuvant therapy duration and an additional 8 weeks of planned delay per institutional standards to appropriately estimate the delay caused by neoadjuvant therapy; second, we conducted sensitivity analyses excluding patients who underwent neoadjuvant therapy to assess for any implications on our results; the results were consistent with no association between time to surgery and survival and postoperative morbidity outcomes.
The study population consisted of patients with rectosigmoid adenocarcinoma (as determined by the operating surgeon), the exact definition of which has been debated recently in the literature.34 Although many surgeons are now calling for strict anatomic definitions, there is no consensus. In this study, we deferred to the operative notes of the operating surgeon to identify which patients had undergone a resection for “rectosigmoid cancer”; however, we could not give a clearer definition beyond this.
Conclusion
For patients treated with curative-intent resection for primary rectosigmoid cancer, no association existed between time to surgery and overall survival, disease-free survival or major 30-day postoperative complications. These results were consistent when time was treated as a nonlinear, linear and dichotomized variable. Our results may reassure health care providers and patients about increasing wait-times, and can provide surgeons and health care administrators some degree of confidence that this patient cohort can withstand moderate delays in treatment without quality of care being compromised. Within specialized cancer centres in a universal health care model, at least for the time-to-surgery durations observed in our cohort, differences in time to surgery are unlikely to affect important clinical outcomes.
Footnotes
Presented as a poster at the Society of Surgical Oncology Annual Cancer Symposium, Mar. 27–30, 2019, San Diego, Calif.
Competing interests: Sami Chadi reports consulting fees and speaking honoraria from Stryker (Endoscopy). No other competing interests were declared.
Contributors: H. Quereshy, S. Chadi and F. Quereshy designed the study. A. Draginov acquired the data, which T. Chesney and K. Guidolin analyzed. H. Quereshy wrote the manuscript, which T. Chesney, K. Guidolin, A. Draginov, S. Chadi and F. Quereshy critically revised. All authors gave final approval of the article to be published.
- Accepted March 14, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.