


Abstract
Background: The use of outpatient health care services by homeless people is low compared to their high level of need; however, it is unclear whether this applies to surgical care. We sought to describe surgical care access among homeless patients in a Canadian tertiary care setting.
Methods: We reviewed the medical records of adult (age > 18 yr) patients with no fixed address or a shelter address who presented to The Ottawa Hospital Emergency Department from Jan. 1, 2013, to Dec. 31, 2014, and required surgical referral. We analyzed the data using descriptive statistics.
Results: A surgical referral was initiated in 129 emergency department visits for 97 patients (77 men [79%], mean age 46.7 yr). Most patients lived in shelters (77 [79%]) and had provincial health insurance (82 [84%]), but only 35 (36%) had a primary care physician. The mean number visits for any reason was 7.9 (standard deviation 13.7) (range 1–106). The majority of surgical referrals (83 [64.3%]) were for traumatic injuries, and the most frequently consulted service (52 [40.3%]) was orthopedic surgery. Just under half (48 [49%]) of referred patients attended at least 1 outpatient appointment, and only a third (33 [34%]) completed full follow-up.
Conclusion: Homeless patients presenting to an emergency department and requiring surgical care were predominantly men living in shelters, most frequently seeking care for traumatic injuries. Current outpatient services may not meet the surgical care needs of these patients, as many do not access them. Alternative approaches to outpatient care must be considered, particularly among high-need services such as orthopedics, to support surgical care access among this population.
Homeless patients often have complex health care needs. They experience more severe acute and chronic health conditions than the general population and have an age-adjusted mortality rate that is 2–8 times that among the general population.1–3 Homelessness includes both individuals and families without access to stable, appropriate housing. On any given day, roughly 1% of the Canadian population is considered chronically or episodically homeless.4,5 In 2013, Ottawa had an average of 6705 people using shelters per day.6 Over one-third (38%) of the Canadian homeless population have self-reported unmet health care needs, and many lack access to primary or preventive health care services.2,7,8 Multiple factors such as difficulty coordinating transport to and from medical appointments, hidden costs in the system, and difficulty accessing health cards and prescriptions contribute to unmet needs.2 As such, the use of outpatient care services among homeless people is low, and the use of emergency services is high, with increased rates of hospital admission compared to the general population.9,10 As a result, homeless patients often access health care services episodically through the emergency department, resulting in health care access that is ineffective for both patients and the health care system.2
The mental health and chronic disease needs of homeless patients are well described, and unique service delivery methods have been developed to support their access to mental health and primary care services.1,11,12 For example, providing housing at hospital discharge improves sustained housing among patients with mental health problems.13 Furthermore, integrating intensive case management with outreach supports or drop-in centre services improves health outcomes for homeless patients with mental health problems, as this targets multiple factors that can affect health and use of health care services.11,14 Coordinated treatment programs for homeless people with concurrent mental illness and substance misuse issues have also been shown to improve health outcomes and care access compared to traditional service delivery models.11
The surgical needs of homeless patients are not well understood. High rates of traumatic and exposure injuries, including traumatic brain injury, burns and frostbite, have been identified in this population. However, the long-term management and outcomes of these and other surgically managed conditions have not been explored.3,15 To better understand and address surgical care access among homeless patients, we sought to describe the surgical presentation and care access patterns within this patient population at our institution.
Methods
Setting
The Ottawa Hospital is a tertiary care hospital in Ottawa, Ontario, with 2 sites (Civic Campus and General Campus) roughly 6 km from the downtown core providing emergency and inpatient services. The hospital provides trauma and tertiary care services as the regional centre for eastern Ontario. Adult patients in Ottawa may also access surgical services at 2 community hospitals not captured within this study.
Data sources
Ethics approval for the study was obtained from the Ottawa Health Science Network Research Ethics Board. This study aimed to identify all homeless patients more than 18 years old who presented to The Ottawa Hospital Emergency Department at the Civic or General campus from Jan. 1, 2013, to Dec. 31, 2014, for whom a consultation to a surgical specialist was initiated. Medical record numbers and emergency department visit diagnoses for all encounters during the study period with patients with no fixed address or with a postal code corresponding to a homeless shelter were extracted by the Ottawa Hospital Health Records Department. We reviewed the list of encounters to ensure that each patient was marginally housed and that a referral to a surgical service was generated, either as an outpatient or as an inpatient.
Surgical services included in the study were general surgery, orthopedic surgery, urology, cardiac surgery, neurosurgery, plastic surgery, otolaryngology, vascular surgery and thoracic surgery. Ophthalmology, oral surgery, and obstetrics and gynecology were excluded from the study as outpatient follow-up in these services is not always in outpatient clinics based at the hospital and therefore may not be recorded consistently in the hospital electronic medical record.
Statistical analysis
All emergency department encounters that generated a surgical referral were included in the analytic data set. We reviewed each chart for patient demographic characteristics, clinical data, referral details, surgical management and outpatient follow-up details for each patient encounter. We reviewed all surgical encounters in the patient record during the 2-year study period, even if no new emergency department visit was initiated. We analyzed patient demographic characteristics and data regarding surgical referral and follow-up using descriptive statistics. We used the χ2 test to compare the likelihood of attending outpatient follow-up between those referred directly by the emergency department physician and those seen by the in-house surgical service and referred for outpatient follow-up. Data analysis was performed with the use of SAS 9.3 software (SAS Institute).
Results
Patient demographic characteristics
An initial list of 2069 encounters was generated for all homeless patients who presented to the emergency department during the study period, of which 429 were from the Civic Campus and 1640 were from the General Campus. A surgical referral was initiated in 129 emergency department visits for 97 patients who met the inclusion criteria. Most patients (77 [79%]) were men (Table 1). The mean age was 46.7 years. Most patients (77 [79%]) were living in a shelter. Only 35 patients (36%) had a primary care physician at the time of referral. Most patients (82 [84%]) had provincial health insurance coverage at the time of their emergency department encounter. The number of emergency department encounters per patient, for any reason, over the study period varied widely, from 1 to 106 (mean 7.9).
Patient demographic characteristics
Patient encounters
The majority (72 [55.8%]) of surgical referrals generated by the emergency department were for immediate assessment by the consulting service in hospital, whereas 52 surgical referrals (40.3%) were referrals for outpatient consultation. For the remaining 5 referrals (3.9%), the patient was admitted to a nonsurgical service but required a surgical referral during the hospital stay. Among the 72 referrals for immediate surgical consultation, the patient was seen by the consulting surgical service in 66 cases (92%). Although surgery was recommended in only 27 patients (28%), the majority of these (21 [78%]) required urgent or emergent operative intervention.
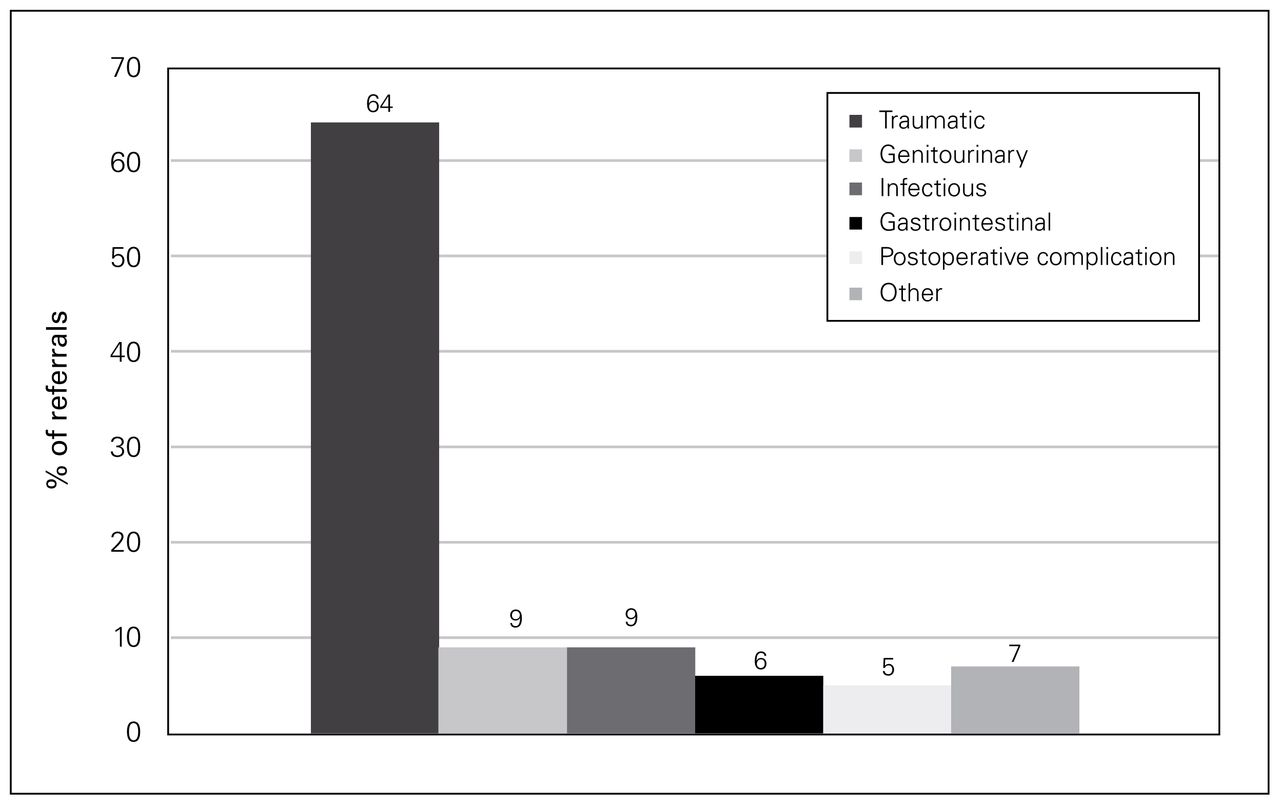
The majority of surgical referrals (83 [64.3%]) were for traumatic injuries, followed by genitourinary (12 [9.3%]), infectious (12 [9.3%]) and gastrointestinal (8 [6.2%]) conditions (Fig. 1). The most frequently consulted surgical service was orthopedic surgery (52 cases [40.3%], followed by plastic surgery (25 [19.4%]), general surgery (12 [9.3%]), urology (12 [9.3%]) and neurosurgery (12 [9.3%]). All other services had less than 5% of the referrals (Fig. 2).
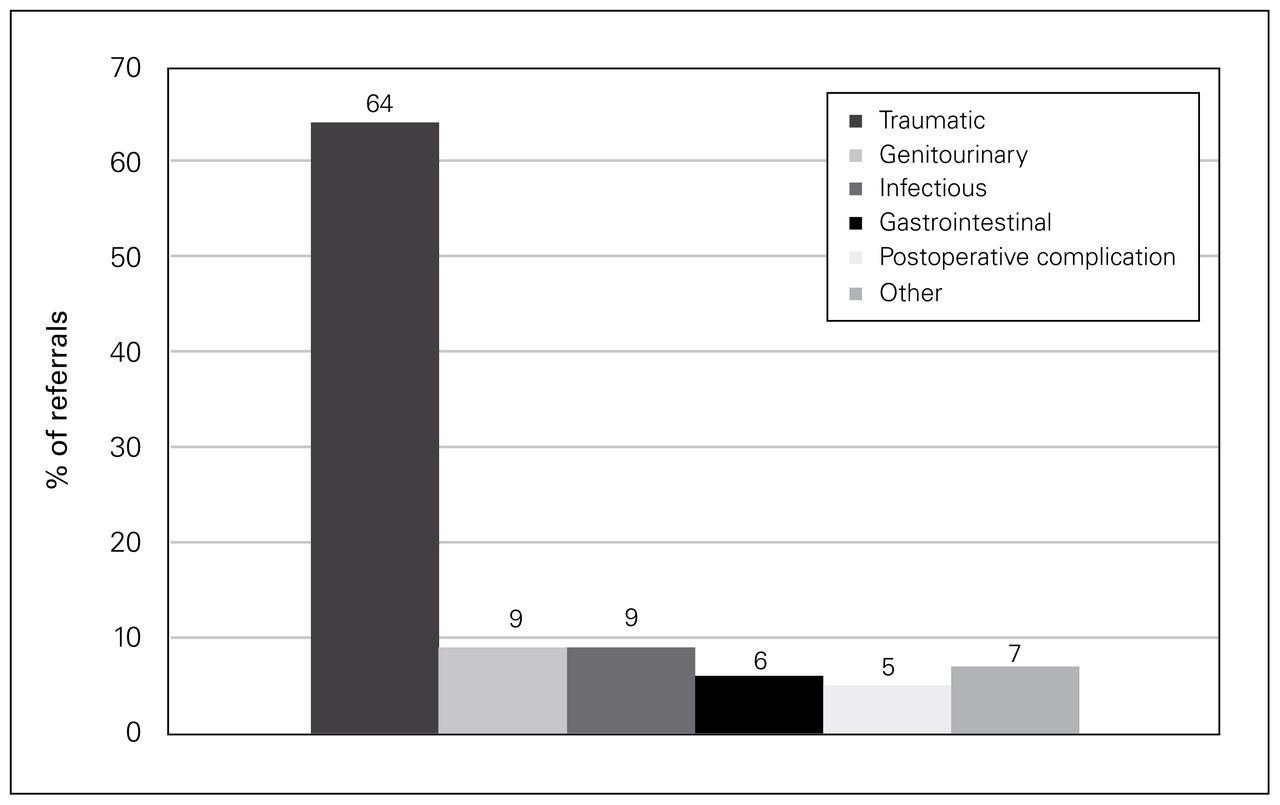
Reasons for surgical referral.

Frequency of referral to surgical services.
Traumatic injuries
Of the 83 surgical referrals for traumatic injuries, 66 (80%) were for fractures: 46 patients (70%) were sent to orthopedic surgery, 19 (29%) were sent to plastic surgery, and 1 (2%) was sent to otolaryngology. Of the 46 patients referred to orthopedic surgery, 25 (54%) were seen in the emergency department, and 21 (46%) were referred for outpatient care. Of the 19 patients referred to plastic surgery, 7 (37%) were seen in the emergency department and 12 (63%) were referred for outpatient care. The 1 patient referred to otolaryngology for a nasal fracture was referred for outpatient care. In total, 32 (48%) traumatic referrals for fractures were seen in the emergency department, and 34 (52%) were outpatient referrals.
Of the 17 surgical referrals for traumatic injuries that were not fracture related, 8 (47%) were for traumatic head injuries referred to neurosurgery, and 5 (29%) were for polytrauma injuries referred to the trauma service. The remaining 4 referrals (24%) represented single-system injuries referred directly to the relevant specialty surgical service (i.e., urology, otolaryngology, thoracic surgery, orthopedic surgery). Most (16 [94%]) of the traumatic referrals unrelated to fractures were seen urgently in the emergency department.
Nontraumatic injuries
Forty-six surgical referrals (35.6%) were for nontraumatic injuries. Two-thirds of these patients (31 [67%]) were seen in the emergency department, 13 (28%) were referred to outpatient care, and 2 (4%) were seen as inpatients. Reasons for referral included peritonsillar abscess, bowel perforation, small bowel obstruction, acute cholecystitis, frostbite, urinary retention and obstruction, critical limb ischemia and wound infection. Three patients (6%) made multiple visits for the same problem (Foley catheter malfunction, infected left hip prosthesis and postoperative hematoma) instead of presenting to outpatient care.
Outpatient follow-up
In addition to the 52 referrals generated by the emergency department physician for outpatient consultation, 53 referrals for surgical follow-up were initiated by the consulting surgical service, either after assessment in the emergency department or following discharge from hospital. Overall, less than half of patients (48 [49%]) attended at least 1 specialist outpatient appointment, and only 33 (34%) completed all follow-up appointments; 16 patients (17%) attended at least 1 follow-up appointment but did not complete treatment and were lost to follow-up. Attendance at 1 outpatient clinic visit was slightly higher among those who were seen and referred by the surgical service in hospital (29 [55%]) than among those referred by the emergency department physician for an outpatient initial consultation (22 [42%]), but the difference was not statistically significant (p = 0.2). In almost two-thirds (42 [64%]) of surgical referrals for fractures, the patient did not complete treatment and was lost to follow-up; 30 (65%) of those referred to orthopedic surgery and 10 (53%) of those referred to plastic surgery did not complete treatment. Twenty patients (43%) referred for nontraumatic injuries did not complete treatment.
Discussion
Our findings provide an overview of the demographic characteristics, disease and injury patterns, and use of outpatient surgical services by homeless patients presenting to the emergency department with surgical disease. Most patients were men who resided in shelters and had provincial health insurance but no primary care physician. The primary reason for surgical consultation was traumatic injury, most commonly requiring orthopedic or plastic surgery care. The majority of nontraumatic referrals were seen in the emergency department, which reflected the urgency of patients’ presenting surgical problems. This is consistent with previous reports that unintentional injuries are a major contributor to emergency department use within homeless populations.3 Homelessness is recognized as a predictor of high rates of emergency department use,16–18 which was also shown in the current study, with a mean of 8 visits per patient over 2 years. However, in our study, few patients used the emergency department for recurrent surgical care access; rather, repeat visits represented care access for nonsurgical health issues.
The poor outpatient surgical follow-up among the homeless population observed in our study is particularly concerning. Over half of patients (51%) referred to outpatient surgical services did not attend any appointments, and only a third completed their full treatment course. Low levels of outpatient care access among homeless populations have also been described in the mental health and medical literature.19 The outpatient follow-up rate in our study was markedly lower than reported surgical follow-up rates within the general population of 82%–87%, with the highest follow-up rates reported among orthopedic surgical referrals.20 Although the majority of surgical service referrals in the present study were to orthopedic surgery, outpatient follow-up with all surgical specialties was markedly poor. Surgical outpatient follow-up is an important contributor to successful patient outcomes, as this is where the need for further intervention may be identified and poor outcomes can be prevented or managed. The majority of surgical referrals were for traumatic injuries, and many of those were for fractures referred to orthopedic and plastic surgery. Thus, improving outpatient follow-up in these areas may be most effective in achieving successful surgical outcomes for such patients. A critical gap in our understanding of surgical outcomes among homeless patients remains, as it is difficult to follow outcomes with such a large proportion of patients being lost to follow-up. Improving outpatient follow-up care among homeless patients is a necessary first step in understanding and improving patient outcomes.
Within the general population, barriers to follow-up include patient choice, physical or social barriers, distance to referral centre, medical insurance coverage, communication failure and consultant’s refusal of the consultation.21–23 Additional barriers to health care access exist for homeless patients, including financial difficulties, lack of knowledge about where to obtain care, lack of child care, long waiting times, perceived discrimination in health care settings and competing priorities for subsistence needs.19,24 It is unclear which factors prevented patients in our study from following through with their surgical care. In addition, transportation is often cited as a barrier to accessing health care services and maintaining medical appointments among the homeless population.25–27 As many homeless patients walk as their primary form of transportation within the community, the 6-km distance between shelters and our hospital campuses may be a significant determinant of care access. Community-centred research in collaboration with community organizations committed to working with homeless patients may help surgeons and health care organizations better understand the barriers to and enablers of outpatient surgical care access and develop strategies for improvement.
Alternative outpatient care models have been successful in mental health and primary care but have not yet been explored in the surgical context.28 These include assertive community treatment teams, which provide intensive multidisciplinary community support through case managers and prioritize flexibility and active outreach rather than clinic attendance.28 Developing partnerships with existing community health care services and outreach programs for homeless patients, such as assertive community treatment programs, outreach clinics and shelters, may inform innovative surgical outpatient care programs. Developing outpatient care models for high-need services such as orthopedic and plastic surgery may improve surgical care access and outcomes among homeless patients.
Limitations
Limitations of this study include a small sample and a single centre review. Emergency department versus direct to outpatient referral patterns may reflect clinical service structures specific to our centre. The approach to medical record identification may have missed homeless patients with postal codes outside those of known homeless shelters, as well as unstably housed patients with a listed postal code but transient housing circumstances. Unstably housed patients are recognized as being difficult to identify within hospital and medical data.27 Access patterns among these patients may be different from those in the study sample. Although poor outpatient follow-up trends were identified, we could not determine specific barriers to outpatient care access from patient records.
Conclusion
Homeless patients who accessed emergency department services for surgical problems were predominantly men living in shelters who presented with traumatic injuries, often fractures requiring orthopedic or plastic surgery referral and follow-up. Patients with nontraumatic injuries often presented with emergent surgical problems. Despite having provincial health insurance, these patients had low rates of outpatient follow-up, which indicates that the current structure of outpatient surgical services does not support their care access. There is a need to identify the barriers that prevent this population from accessing care so that emergency departments and surgical services can appropriately develop alternative approaches to care delivery in order to provide reliable surgical follow-up tailored to the unique care access needs of homeless patients. A prospective study of homeless and marginally housed patients as they are referred to surgical services may better allow identification of care access barriers. Developing partnerships with community organizations may also provide important insights, as well as avenues for care structures that better meet the surgical needs of this population. Better access to follow-up care among homeless patients is required to enable good surgical outcomes.
Acknowledgements
The authors acknowledge The Ottawa Hospital Health Records Department for its assistance in obtaining patient charts and creating an initial database.
Footnotes
Competing interests: None declared.
Funding: This research was supported by a 2014 Phoenix Fellowship from Associated Medical Services, which was used to obtain patient charts from The Ottawa Hospital health records database.
Contributors: All authors designed the study and acquired and analyzed the data. L. Zuccaro, C. Champion and S. Bennett wrote the article, which all authors reviewed and approved for publication.
Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the official views of Associated Medical Services.
- Accepted February 15, 2018.
References

{kind=link}
{kind=link}
Article tools





