


Abstract
Background: Open iliac bone harvesting techniques can result in significant complications and residual morbidity. In reconstructive procedures where a small volume of autogenous cancellous bone graft is required, a minimally invasive technique for bone harvesting applied at the mid-iliac crest has been deemed satisfactory. We sought to assess the application of a well-established surgical technique to procure adequate volume of autogenous cancellous iliac bone graft with minimal trauma to adjacent structures.
Methods: We retrospectively reviewed the cases of patients who underwent a minimally invasive transcrestal mid-iliac bone graft procurement technique between May 2003 and December 2007. The technique was performed using a 3.5-mm Steinmann pin as a trocar and a 4.5-mm AO drill sleeve as a trephine. We administered a questionnaire, either in the clinic or by mail, to assess a number of parameters, including postoperative pain, dysthesia, parasthesia, status of the donor site wound and patient satisfaction.
Results: Of the 37 consecutive patients who underwent the procedure, data from 26 patients were available for assessment. Donor site pain resolved within a few days of the surgery, and none of the patients experienced symptoms of chronic pain. At the final review, none of the patients reported any unpleasant signs and symptoms related to the residual scar.
Conclusion: We recommend that the described minimally invasive trephine method be used when a small cancellous bone graft is needed. We found that patient morbidity was significantly lower with the trephine harvest technique than with open bone harvesting methods at the anterior iliac crest.
With the emergence of newer reconstructive techniques, the demand for bone grafting as repair and replacement material or extension of the native anatomy has increased over the last decade. The quality and quantity of bone graft material needed is largely dictated by the indication for its demand at the recipient site. Harvesting of autogenous bone graft is often accompanied by significant morbidity at the donor site. Weikel and Habal1 reported a 9.4% incidence of donor site complications, including chronic wound pain and hypersensitivity, buttock anesthesia and meralgia parasthetica. Other studies have since reported such complications, particularly with classic large-incision, open techniques for bone graft harvesting from anterior and posterior parts of the iliac crest2,3 and with minimally invasive methods.4 For optimum osteoconductive, osteoinductive and osteogenic properties, autogenous cancellous bone procured from the ilium is preferred when load-bearing structural support is not required.5,6 Experience suggests that when less than 50 mL of cancellous bone graft material is required for the recipient bed, harvesting from the anterior half of the ilium is preferred.7,8
Open methods are associated with unavoidable short-and long-term chronic complications despite careful surgical practices. New, less invasive techniques of bone graft harvesting have been developed to decrease donor site morbidity.9–11
To harvest bone graft, Saleh12 recommended using a Meunier trephine, originally intended for bicortical iliac bone biopsies, which resulted in less substantial surgical trauma and postoperative pain. Others have also used a trephine to harvest bone specimens for the purposes of biopsy and bone graft with minimal morbidity.13–15 Kreibich and colleagues16 and McGurk and colleagues17 demonstrated the safety of a trephine in other fields of surgery as well. Thus, trephination has been reported to minimize morbidity at the anterior ilium for harvesting cancellous bone.
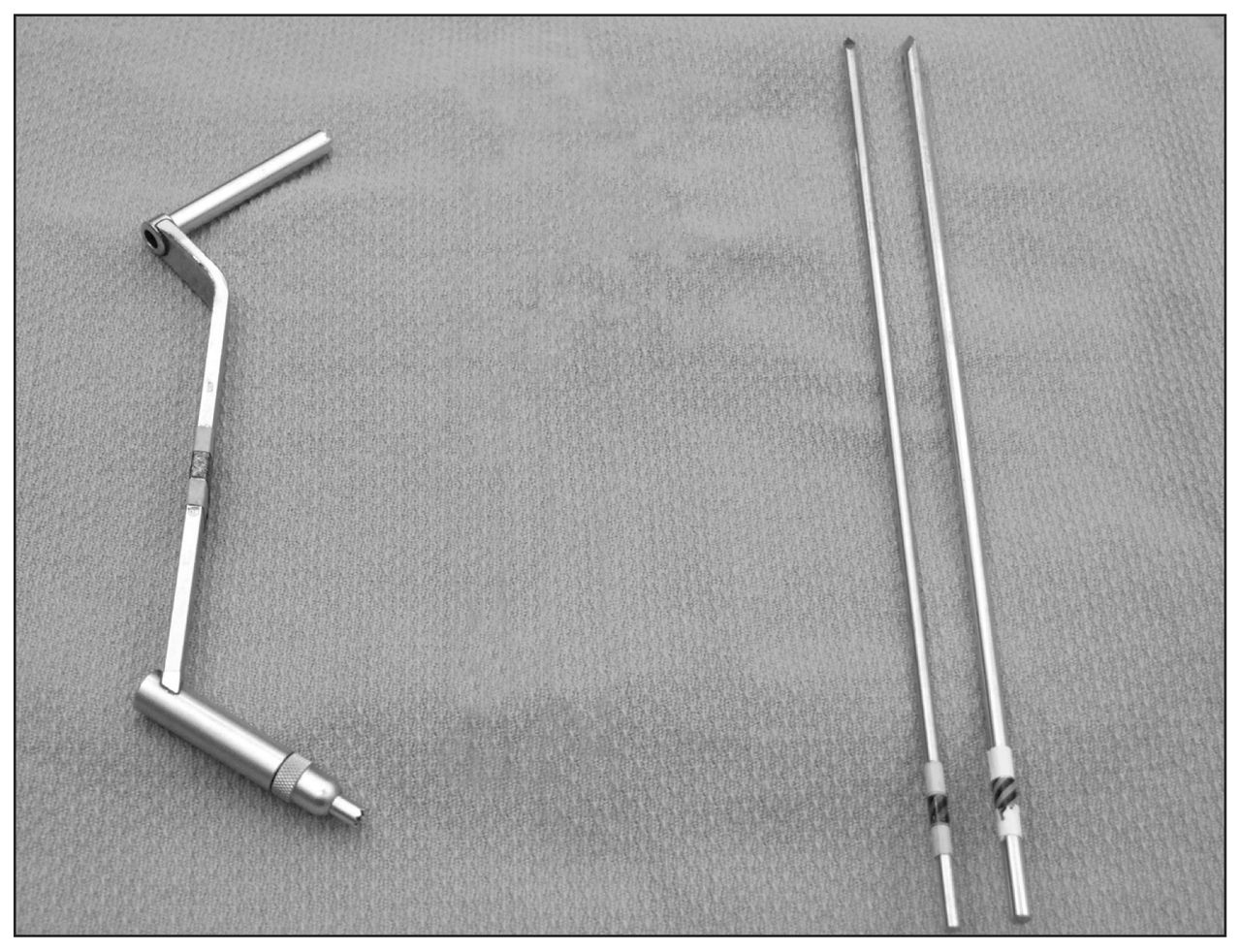
The objective of our study was to assess the application of a well-established surgical technique to procure an adequate volume of autogenous cancellous iliac bone graft with minimal trauma to adjacent structures. The procedure can easily be performed by inserting a bone pin through the iliac crest in exactly the same manner as for the application of a pelvic external fixator pin. For this purpose, we used a readily available unthreaded Steinmann bone pin and a drill sleeve from a standard large fragment AO fracture fixation set (Fig. 1) as a trocar and trephine, respectively, without incurring any additional expense. By paying due attention to the anatomy of the iliac wing, the procedure we describe causes minimum short-term discomfort and no long-term morbidity at the donor site.
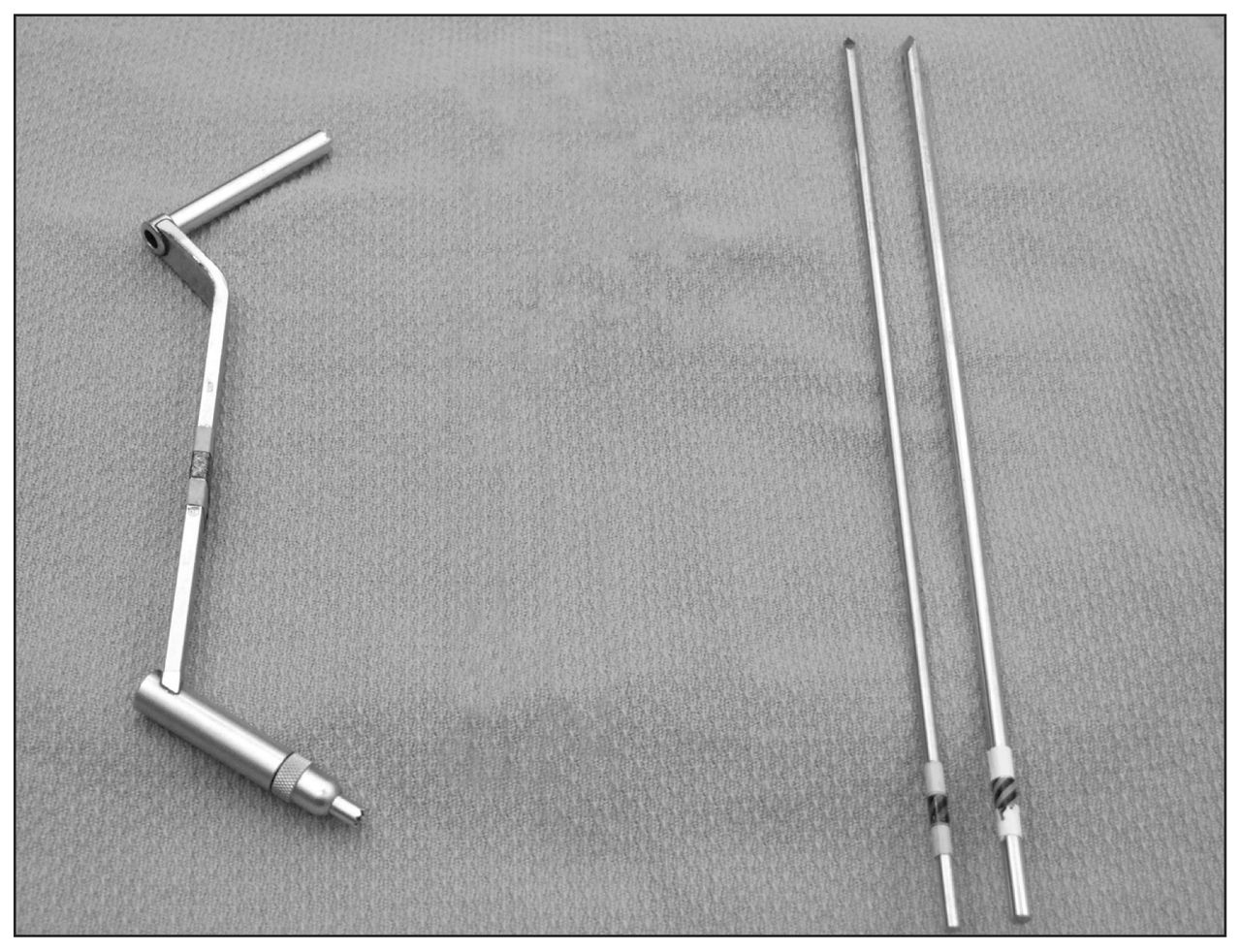
Instruments used in the minimally invasive procedure: a 4.5 AO drill sleeve and various sizes of Steinmann pins.
Anatomic consideration
The ilium is the largest of the 3 bones that make up the innominate bone of the pelvis: the thin concavo-convex ala or wing ends above the iliac crest, which curve between the anterior and posterior superior iliac spines. The crest is subcutaneous, but the remaining parts are covered by muscles. The iliac crest is palpable and serves as the anchoring point for the muscles of the abdominal wall, specifically the internal and external oblique muscles and the transverse abdominus. In adults, the thickest portion of the crest is about 5 cm posterior to the anterior superior iliac spine, where the crest widens. The wide portion is the uppermost extent of the gluteal pillar, a thickening of bone that courses from the upper acetabulum to the iliac crest and is believed to be important in load transference from the lower extremity to the pelvis. The junction of the abdominal and gluteal muscles forms a musculoperiosteal fascia to gain insertion atop the whole length of the iliac crest.
The anatomic course of the lateral femoral cutaneous nerve (LFCN) is in close proximity to the anterior superior iliac spine (ASIS) and is easily injured when obtaining bone grafts from the anterior ilium. In most adult anatomic specimens, the LFCN crosses the region either ventral to the ASIS within the substance of the inguinal ligament or within 2 cm dorsolateral to the ASIS. However, in up to 9.9% of specimens, the nerve takes an anomalous course over the crest up to 5 cm dorsolateral to the ASIS.18
Donor site complications may be prevented by giving due consideration to the anatomy of the iliac crest and by techniques that cause the least amount of disturbance to the associated structures.
Methods
We retrospectively reviewed the cases of 37 consecutive patients who were referred by 2 oral surgeons (B.E.H. and E.M.G.D.) for bone graft harvesting between May 2003 and December 2007. The indications for autogenous bone graft were mostly alveolar defects and cleft palate. Autogenous cancellous bone graft material was procured from the mid-ilium. The surgical technique, described in the next section, was devised and performed in all patients by the senior surgeon (P.C.M.). One surgeon (H.S.G.), who was not involved with the surgery, reviewed the cases of all the available patients from the series. The following parameters were recorded at the final review using a questionnaire administered either in the clinic or by mail:
duration and degree of postoperative pain at the surgical site;
duration of pain and limp associated with ambulation;
dysthesia in the form of itching, burning and hypersensitivity over the scar;
parasthesia in the distribution of the lateral femoral cutaneous nerve of the ipsilateral thigh;
satisfaction with the cosmetic appearance of the residual scar;
satisfaction with the primary surgery (i.e., was the discomfort from the donor site worthwhile?);
willingness to undergo the same procedure for bone graft harvesting from the iliac bone if needed;
willingness to recommend the minimally invasive approach to other patients who need bone graft;
need for overnight stay in hospital; and
status of the donor site wound at the final clinical examination, including distance from the ASIS and the length and width of the residual scar.
The Research Ethics Board of the McMaster University Medical Centre approved our study protocol and we obtained informed consent from all participants.
Surgical technique
In all our patients, the primary oral surgery procedure required general anesthesia and supine positioning, presenting the anterior ilium for easy access. To enhance the presentation of the iliac crest and shift the bulk of the abdominal wall, a bolster was placed under the ipsilateral buttock. The regional skin was prepared with solution of povidone and draped to expose the anterior half of the crest to easily define the landmarks: the ASIS, the iliac tubercle and the lateral and medial edges of the iliac crest. Depending on the skeletal maturity of the patient (20–50 mm dorsolateral to the ASIS), either the maximum width of the iliac crest (prepubescent patient) or the iliac tubercle (adult patient) was palpated, and overlying skin and deeper tissues were stabilized between the thumb and index finger on the nondominant hand. A 10 mm–long skin incision, 10 mm distal to the iliac margin, was made and then mobilized over the crest. Blunt dissection was carried out using a Steinmann pin to reach the iliac crest. Medial and lateral margins of the crest were defined by using the tip of the pin to locate the centre of the crest. The trocar tip of the pin was then engaged into the iliac crest with a gentle blow of a hammer and was driven slightly in between the 2 tables of the iliac bone (Fig. 2). In prepubescent patients, this method never split the iliac apophysis.

Placement of the drill sleeve between the inner and outer tables of the iliac bone.
A 4.5-mm drill sleeve, as the harvesting trephine, was passed over the positioned Steinmann pin as its guide into the iliac wing. The trephine was carried deeper into the cancellous bone between the inner and outer plates with a twisting motion. The surgeon determined the depth of penetration. To break the bone dowel, the handle of the sleeve was turned slowly back and forth through an arc of motion of about 360° to cause a fatigue fracture to release it. The sleeve was removed by its handle, carrying the bone graft along with the guiding pin. The graft dowel was extracted by plunging the pin through the sleeve into a container (Fig. 3). The harvested bone was often compacted and difficult to extract. We found that using a Steinmann pin the same size as the cannula as a guide causes binding of the cancellous bone plug and the barrel of the cannula, whereas using a pin the next size smaller facilitates the retrieval of the bone plug from the barrel.

Delivery of the harvested bone graft dowel using the smaller Steinmann pin as a plunger.
Usually, 3 or more additional dowels were harvested by reinserting the trephine with the guide in anterior and oblique posterior directions through the existing perforation in the iliac crest at an angle of about 45° with twisting movements. Once again, the trephine sleeve was gently twisted and levered to break the core at its base. If the amount of collected graft material was felt to be insufficient for the recipient bed, with or without extending the existing skin incision, a second perforation was made in the crest. Rarely, a fresh second skin incision further dorsal to the first incision was made, and the procedure was repeated. For incisions of less than 1 cm, the wound was closed with a full thickness suture of 3–0 nylon, and a Micropore dressing was applied. Sutures were removed 10–14 days later. There was no need for a bone defect filler material, hemostatic plug, any type of drain or pressure dressing because there was no deep muscle dissection causing hematoma formation. Occasional breech of the iliac wall occurred.
Results
Of the 37 patients who underwent the procedure, 11 were lost to follow-up leaving data for 26 patients available for assessment. Thirteen of these patients completed the questionnaire in the clinic and 13 responded to the same questionnaire by mail. Of the 26 patients included in our analysis, 18 were male (age range 10–70 yr) and 8 were female (age range 11–77 yr). The bone graft came from the left iliac crest in 24 patients and from the right in the remaining 2 patients. The postoperative follow-up period was 3–57 months.
The volume of the bone graft obtained was not measured formally. On each occasion, the amount procured was to the satisfaction of both the oral surgeons for a given indication.
Table 1 summarizes the clinical results of the 26 patients available for assessment. None of the patients had to stay overnight in hospital owing to bone graft donor site symptoms. The duration of pain experienced at the donor site was 0–56 days. Four patients reported no pain at all postoperatively, 3 had complete resolution of the pain within the first 24 hours, 11 in 7 days and the remaining 8 within 8 weeks (56 d). Thus, 69.2% were completely without pain in 7 days. The mean intensity of pain severity on a scale of 0–10 (10 being severe) was 4 (range 0–9). Among the 13 patients evaluated in the clinic, the mean length of the residue from skin incision was 11.9 (range 7–20) mm, the mean width was 1.7 (range 1–3) mm, and the mean distance from the anterior superior iliac spine was 26.3 (range 6–46) mm. Gait disturbance in the form of discomfort and slight limp on ambulation was reported by 11 (42.3%) patients, and the mean duration was 14 (range 2–56) days. Apart from itching during wound healing reported by 4 patients, no other symptoms were reported.
Postoperative characteristics of patients who underwent a minimally invasive autogenous cancellous bone graft procedure
At the time of the final review, none of the patients reported any symptoms suggestive of meralgia parasthetica at any time during the recovery period, and all patients had complete resolution. There were no postoperative wound complications. There were no hyperpigmented, hypertrophic or keloid scars either observed or reported. All 26 patients were completely satisfied with the cosmetic appearance of their residual scar. Three of 26 (11.5%) patients were unwilling to have the bone graft harvesting procedure repeated in future. With the exception of those 3 and 1 other patient who did not answer the question, the remaining patients were willing to recommend the minimally invasive approach to other patients who need bone graft.
Operative reports for all 37 patients who underwent this minimally invasive procedure were reviewed for intraoperative events. In all patients, blood loss during the surgery was insignificant (i.e., requiringing 5 or fewer 4 × 4–gauge sponges). In 1 patient, the procedure was abandoned because on each penetration the trephine returned empty. In 2 patients, the surgeon decided to make a second iliac wing penetration further dorsally using the same incision to harvest extra volume of bone to satisfactorily complete the reconstructive procedure.
Discussion
The pioneering study by Urist and McLean19 described the osteoinductive properties of autogenous bone. Compared with allografts and alternative nonbiologic bone substitutes with added high cost, autogenous cancellous bone provides superior osteogenic properties and lacks potential problems of immunologic inflammatory reaction leading to rapid resorption of the graft.20
The safety and benefit of trephines has been demonstrated by Kreibich and colleagues,16 who showed that the percutaneous sampling of bone, when compared with open procedures, resulted in significantly reduced pain in general and when walking, fewer sensory disturbances and less local tenderness. The most common donor site complications for the anterior ilium described in the literature are acute and chronic wound pain, hematoma formation, infection, lateral femoral cutaneous nerve injury, gait disturbances, cosmetic dissatisfaction and, rarely, anterior iliac bone fracture and abdominal hernias resulting in a prolonged stay in hospital related to large incisions for open techniques.2,3,21,22 Younger and Chapman3 reported rates of major and minor complications of 5.3% and 25.0%, respectively, for the anterior iliac crest donor site. In a retrospective review of 414 consecutive patients, Arrington and colleagues2 reported rates of 10.0% for minor and 5.8% for major complications, including 2 iliac wing fractures and 3 LFCN injuries. Goulet and colleagues23 reported rates of 37.9% for chronic pain, 12.6% for gait disturbances lasting 6 months and 1.2% for keloid scars. We infer that with larger exposure and associated greater soft tissue dissection the reported complications can be expected.
In adults, there exists a “safe anatomic zone” of about 35 mm in length, 10 mm in width and 30 mm in depth at the site of the iliac tubercle to procure a cancellous bone graft with a trephine similar to the kind used in the present study. With the present technique, injury to the LFCN is prevented by choosing not to make the skin incision less than 30 mm posterior to the ASIS18,24 and by bluntly dissecting over the iliac crest. There is no danger of causing stress fracture or avulsion fracture of the ASIS25 because, after the initial careful perforation of the iliac crest with the Steinmann pin, the trephine guided over it is carried to its final depth with a twisting motion between the inner and outer tables without compromising the biomechanical strength of the anterior ilium.
The outcomes in the immediate postoperative period of our minimally invasive technique for procuring autogenous cancellous bone graft are consistent with those reported in other similar studies.4,26 After a follow-up period of 2–56 months, none of our patients had any unpleasant signs or symptoms. All those who reported were completely satisfied with the cosmetic appearance of the residual scar.
No specialized instruments were bought for the autogenous iliac bone graft procedure. A reusable 4.5-mm drill sleeve from the existing standard large fragment AO fracture fixation set and a commonly available 3.5-mm Steinmann pin were used without incurring any extra instrument cost to the hospital.
It is clear that most of the complications encountered during harvesting of bone graft from the iliac crest can be prevented by using a safe, minimally invasive technique. As in any other minimally invasive surgery, to prevent long-term morbidity at the iliac crest bone graft donor site, it is important to be cognizant of relevant anatomic land marks and possible anomalies of important structures that are in danger of being injured. When a small amount of cancellous bone graft is required, we recommend that a trephine method such as ours be considered. An adequate volume of bone graft can be procured to the satisfaction of the primary surgeon for the given indication of a reconstructive procedure. If additional volume of bone is required, a second perforation of the iliac crest may be made more dorsally by repeating the procedure. As shown in this and other studies, morbidity is consistently less with a trephine harvest technique than with open bone harvesting methods at the anterior iliac crest. Careful application of the trephine does not compromise the tricortical architectural integrity of the pelvis, thereby minimizing morbidity at the donor site.
Footnotes
Competing interests: None declared.
Contributors: Dr. Harnett and Ms. Roberts designed the study. Dr. Missiuna developed the surgical technique. Drs. Missiuna, Gandhi and Harnett acquired the data. Drs. Gandhi, Farrokhyar, Harnett and Dore analyzed the data. Dr. Gandhi wrote the article. Drs. Missiuna, Farrokhyar, Harnett and Dore and Ms. Roberts reviewed the article. All authors approved its publication.
- Accepted January 12, 2011.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.