


Retrorectal cystic hamartomas (RCHs) or tailgut cysts are rare congenital lesions. Typically, they present as presacral masses. Associated malignant change is rare; only 16 such cases have been reported in the literature. We describe the clinicopathologic features of a new case of RCH associated with malignant transformation.
Case report
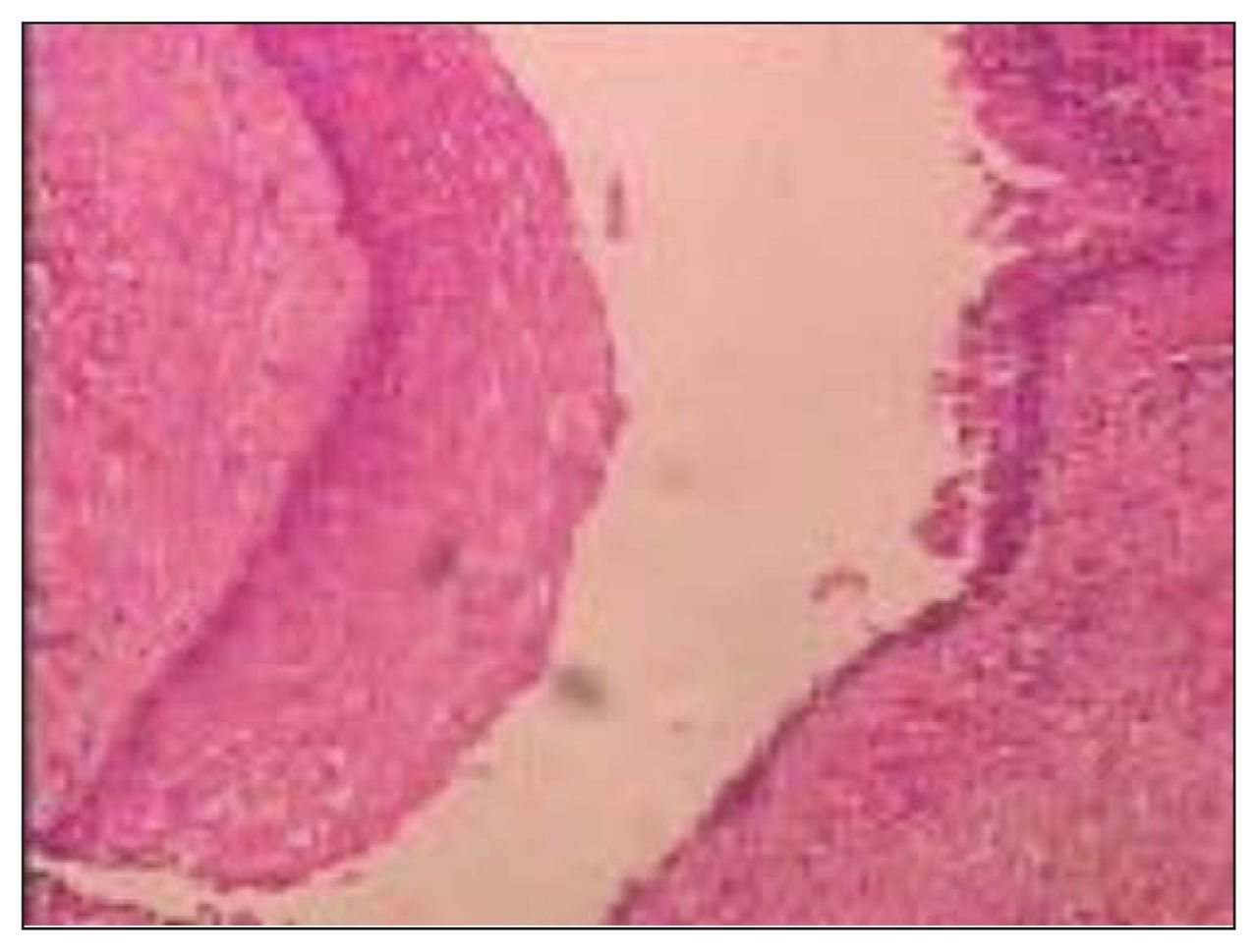
A 49-year-old woman presented with pelvic and perineal pain of 6 months’ duration. On physical examination, there was no abnormality. Digital rectal examination showed a nontender, extrinsic, well-defined presacral mass compressing the rectum. Sigmoidoscopy revealed no mucosal abnormalities. Routine laboratory test results were within normal limits. Abdominal computed tomography (CT) demonstrated a well-demarcated hypodense, bilocular cystic lesion, 15 cm in size, in the presacral region to the right of the midline (Fig. 1). At laparotomy for excision of the lesion, we found that the mass was adherent to and not easily separated from the rectum and surrounding pelvic wall. The surgical specimen consisted of 3 fragments of fibrofatty tissue. The cyst lining was focally hemorrhagic, and the cyst contained clear fluid. Microscopic examination revealed that the wall comprised smooth muscle lined by a variety of epithelia (stratified squamous, stratified ciliated columnar and transitional cells. There was a focus of malignant transformation corresponding to adenocarcinoma (Fig. 2).

Computed tomography scan showing a multilocular, cystic, hypodense retrorectal lesion.

Microscopic examination revealed the cyst wall comprising smooth muscle lined by a variety of epithelia, including stratified squamous, stratified ciliated columnar and transitional cells.
The patient’s postoperative recovery was uncomplicated. She received adjuvant radiochemotherapy with MacDonald protocol (5-fluorouracil and folinic acid [FUFOL] with concomitant radiotherapy [45 Gy]) for 12 weeks. She was alive with no recurrent disease 4 years after surgery.
Discussion
The retrorectal (presacral) space is one bounded anteriorly by the rectum, posteriorly by the sacrum, superiorly by the peritoneal reflection and inferiorly by the levator ani and coccygeus muscle. Teratomas are the more common lesions in children, whereas in adults, chordome and developmental cysts are more frequent. 1–3 In the literature, various terms have been used to describe RCHs, including cyst of the postanal intestine, tailgut cyst, mucus-secreting cyst, simple cyst, retrorectal cyst and enterogenous cyst.1,2,4 They are believed to arise from the remnants of the embryonic hindgut. Retrorectal cystic hamartomas are 3 times more common in women than men. They can be detected at any age, including infancy.2,3
Nearly half the patients are asymptomatic; the remainder present with symptoms of a mass effect or pain, as in our patient. Investigations include ultrasonography, endosonography, endoscopy, CT or magnetic resonance imaging. The cyst may be unilocular or multilocular and range in diameter from 2 to 12 cm. A variety of epithelial linings may be seen, including stratified squamous, cuboidal, transitional, stratified columnar, mucinous or ciliated columnar cells. Interrupted bundles of smooth muscle are present.1,3,5
The differential diagnosis of RCH includes rectal duplication cyst, cystic teratoma, and dermoid and epidermoid cyst.3 Epidermoid and dermoid cysts are usually unilocular and are lined by stratified squamous epithelium. Dermal appendages are present in dermoid cysts. Duplication cysts are unilocular and are lined by epithelium similar to that of the gastrointestinal and respiratory tracts. The potential for infection, recurrent perineal fistulas and malignant transformation emphasizes the risk associated with early incomplete surgical excision of these lesions. Complete surgical resection is the therapy of choice.1,3,5
Malignant change as a rare complication has been described occasionally. In an extensive search of the literature, Tampi and colleagues1 found only 16 cases with malignant transformation. The largest series of 53 cases was reported by Hjermsted and Helwig4 from the Armed Forces Institute of Pathology; they found only 1 case associated with malignant transformation. Prasad and colleagues3 collected 12 cases of RCH with malignant transformation reported in the literature, 7 with adenocarcinoma and 5 with carcinoid.
Our patient received adjuvant radiotherapy and chemotherapy without evidence that this protocol would improve the prognosis.
Conclusions
Retrorectal cystic hamartoma is an uncommon entity that should be included in the differential diagnosis of a retrorectal mass. Complete surgical excision is the therapy of choice. Malignant transformation, although unusual, may be focal, so meticulous examination of the gross mass and thorough samplings are important.
Footnotes
Competing interests: None declared.
- Accepted March 13, 2008.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.