


Abstract
Background: Continuity of primary care (CPC) improves patient well-being, but the association between CPC and surgical outcomes has not been well studied. The numbers of joint replacement procedures are expected to rise considerably in the coming years, so it is crucial to identify factors related to successful outcomes. The purpose of this study was to examine the association between CPC and emergency department (ED) visits after knee and hip replacement surgery.
Methods: Physician claims and hospital data from 2005 to 2020 in Nova Scotia were used in this retrospective study. To measure CPC, we used the Modified Modified Continuity Index (MMCI), which is the number of primary care providers adjusted for the total number of visits. The outcome was ED visits within 90 days of discharge. Logistic regression was used to test for associations between MMCI and the probability of an ED visit.
Results: There were 28 574 knee and 16 767 hip procedures in the data set; 13.9% (95% confidence interval [CI] 13.5%–14.3%) and 13.5% (95% CI 13.0%–14.0%) of the patients, respectively, had an ED visit within 90 days. For patients who underwent knee procedures, the mean MMCI was 0.868 (95% CI 0.867–0.870); 10.7% (95% CI 10.4 %–11.1 %) had perfect continuity of care. For patients who underwent hip procedures, the corresponding measures were 0.864 (95% CI 0.862–0.866) and 13.5% (95% CI 13.0%–14.0%). There was a statistically significant negative association between greater continuity of care and the probability of an ED visit after controlling for confounders.
Conclusion: Having multiple primary care providers before surgery increased the likelihood of negative outcomes following knee or hip replacement surgery compared with having a single provider. Presurgical conversations should include primary care history to improve postsurgical outcomes.
Access to a primary care provider is an important indicator of quality health care. Continuity of primary care (CPC) has been identified as a central component of primary care provision and incorporates the concepts of coordination, integration, patient-centred care and case management.1 A key benefit of CPC is to build trust between the physician and patient, which improves communication and increases compliance and shared decision-making.2,3
For patients undergoing surgery, primary care providers play a crucial role along the continuum of care. Osteoarthritis, the most common reason for joint replacement surgery, often takes many years to develop4 and requires frequent family medicine visits. As well, lengthy follow-up for postsurgical care supports the notion that primary care provision is vital to surgical recovery.5 An emergency department (ED) visit after a surgical procedure can be an indication of inappropriate care before, during or after surgery.6–8 Hip and knee replacement procedures are commonly associated with intense pain both before and after surgery, which has been shown to increase the likelihood of an ED visit following surgery.9 Ensuring patients’ readiness for surgery and providing follow-up care frequently are the responsibility of the primary care provider, suggesting CPC is especially relevant for this population. The objective of this study was to test for associations between CPC and the probability of an ED visit within 90 days of hip or knee replacement.
Methods
The study population was all patients who underwent non-emergency hip and knee procedures from 2005 to 2020 in Nova Scotia as selected from the hospital Discharge Abstract Database and the National Ambulatory Care Reporting System, which includes both inpatient and out-patient procedures. Given that the COVID-19 pandemic resulted in extraordinary health care system circumstances, only cases before the pandemic were included. Procedures were identified using Canadian Classification of Health Interventions codes. Ethics approval was given by the Nova Scotia Health Authority Research Ethics Board.
The study outcome was any ED visit in the 90 days after discharge. The Modified Modified Continuity Index (MMCI)10 was used to measure CPC; it is an index representing the number of primary care practitioners adjusted for the total number of visits. A higher MMCI value signifies increased continuity; the maximum value of 1 indicates a single provider for all visits. If every visit was to a different provider, the MMCI score would be very near zero. A higher number of visits for the same number of providers will increase the MMCI. For example, 6 primary care visits across 2 providers will result in a higher MMCI than 4 primary care visits across 2 providers. A lower score probably indicates that patients do not have a regular provider and are accessing care at walk-in clinics, mobile care units and the like. The MMCI was calculated for each individual using physician claims data in the 3-year period before surgery, excluding those who had fewer than 3 primary care visits.
Statistical analysis
Associations between CPC and the probability of a 90-day ED visit were tested using unadjusted and adjusted logistic regression to control for confounding factors. Covariates were selected on the basis of a review of the literature, clinical expertise and what was available in the data. The factors that were included were age, sex, year of surgery, comorbidities, length of stay, hospital where the hip or knee surgery was performed, admission from home, neighbourhood income, a blood transfusion indicator and distance from home to hospital. Also modelled as a covariate was an indicator of any visit to the ED in the year before surgery. This variable was included so that the results would better reflect the likelihood of ED visits beyond those that may have occurred in the absence of surgery because evidence suggests there is a link between CPC and ED use in general.11–13 Some individuals may be more inclined to go to the ED irrespective of having had surgery. Consequently, the addition of any presurgical ED visit in the models targets the effect of surgery more precisely.
The MMCI was modelled as a continuous variable whereby the index was multiplied by 100 to obtain a more meaningful interpretation of the odds ratios (ORs). A second model was run in which the MMCI was replaced by a 1/0 binary variable where 1 signified a perfect score of 1. This model compared the probability of an ED visit for those who saw only 1 provider for all visits to the probability of an ED visit for all others. Analyses for knee and hip procedures were run separately. To give context to the effect size of changes in the MMCI, probabilities of an ED visit were calculated.
Given that logistic regression fits the data to a nonlinear function, the change in the probability of an ED visit given a change in the MMCI will vary depending on the values of the covariates. As such, the probability was calculated for a base case scenario whereby categorical variables were set to 0 (i.e., reference categories were applied) and continuous variables were set to their mean values. Specifically, the base case was a man aged 60–69 years with no comorbidities who had surgery at the reference hospital, had an average household neighbourhood income and lived the average distance to the hospital. He had not had a visit to the ED in the year before surgery and had had a single provider for all primary care visits in the previous 3 years. Probabilities were then calculated for this individual under 3 separate scenarios: he had multiple primary care providers, he was older and he had a comorbidity. All other characteristics were held constant. SAS version 9.4 was used for all analyses.
Results
There were 28 574 knee and 16 767 hip procedures included in the analysis data set, with 13.9% (95% confidence interval [CI] 13.5%–14.3%) and 13.5% (95% CI 13.0%–14.0%) of the patients having had an ED visit within 90 days of surgery, respectively. The mean MMCI was 0.868 (95% CI 0.867–0.870) for knee cases and 0.864 (95% CI 0.862–0.866) for hip cases; 10.7% (95% CI 10.4%–11.1%) of knee cases and 13.5% (95% CI 13.0%–14.0%) of hip cases had a perfect continuity score of 1.
The ORs for the unadjusted and adjusted models are presented in Table 1. There was a negative association between the MMCI and the probability of a 90-day ED visit after discharge for both knee and hip cases. For the unadjusted models, every unit increase in the MMCI (× 100) decreased the probability of an ED visit by 1.3% (95% CI 1.0%–1.5%) and 0.9% (95% CI 0.6%–1.2%) for knees and hips, respectively. After adjusting for confounders, the effect of the MMCI decreased but remained statistically significant. For both knees and hips, an increase in the Charlson Comorbidity Index score, age, year of surgery, anemia and blood transfusion increased the likelihood of an ED visit. Notably, an ED visit in the year before surgery more than doubled the chance of an ED visit 90 days after discharge (OR 2.44, 95% CI 2.26–2.62 for knees; OR 2.01, 95% CI 1.82–2.22 for hips).
Association between emergency department visits following knee or hip replacement surgery and continuity of primary care
The binary measure of CPC indicating all visits to a single provider (i.e., an MMCI value of 1) was associated with a decrease in the likelihood of a 90-day ED visit. The odds of a 90-day ED visit for patients with a knee replacement who had had 1 primary care provider in the previous 3 years was nearly 40% lower than for those who had had multiple providers; among patients with a hip replacement, the odds was 35% lower for those who had had 1 primary care provider in the previous 3 years than for those with multiple providers. The association remained statistically significant after controls were included in the models, although the magnitude was reduced (Table 2).
Association between emergency department visits following knee or hip replacement surgery and perfect continuity of primary care (1 primary care provider)
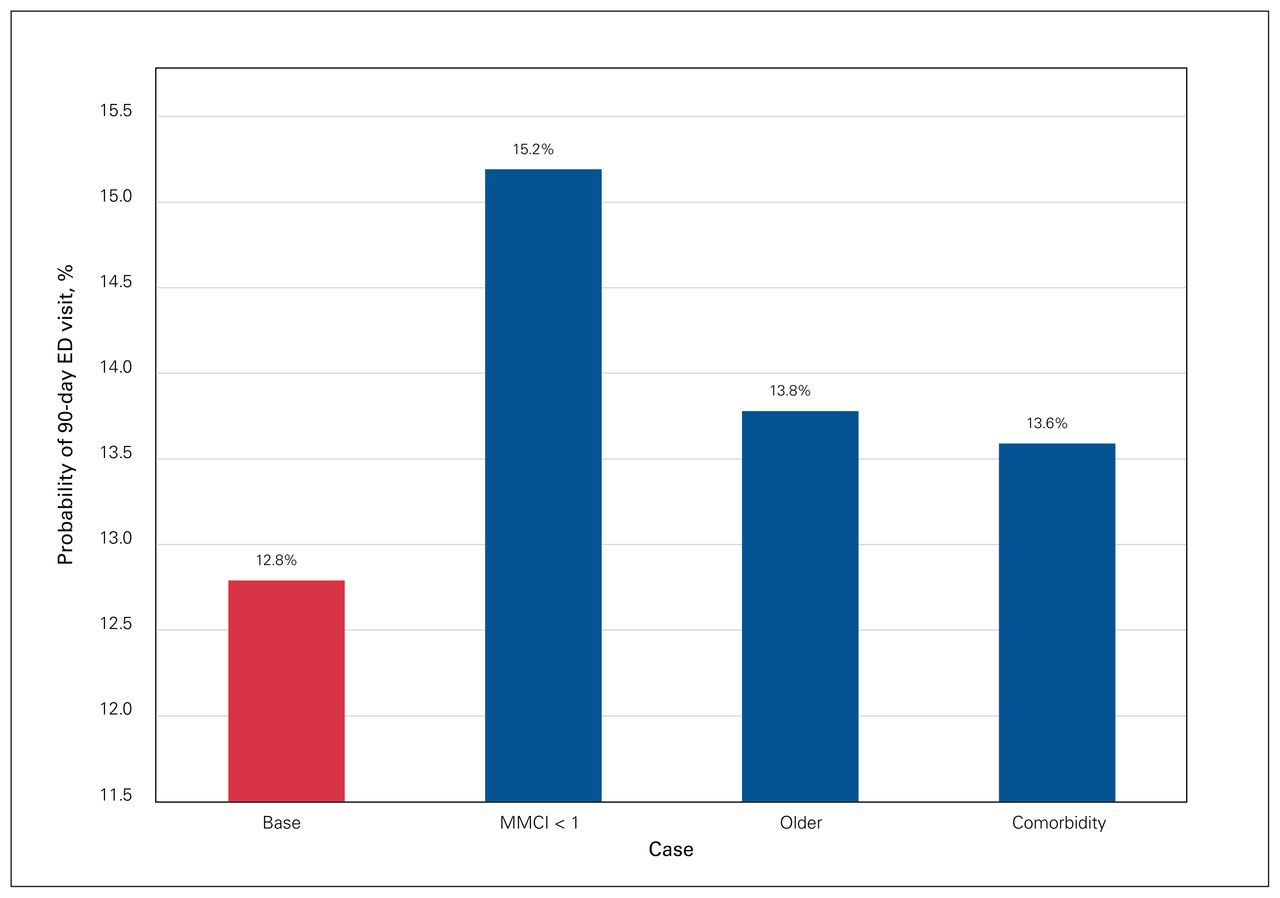
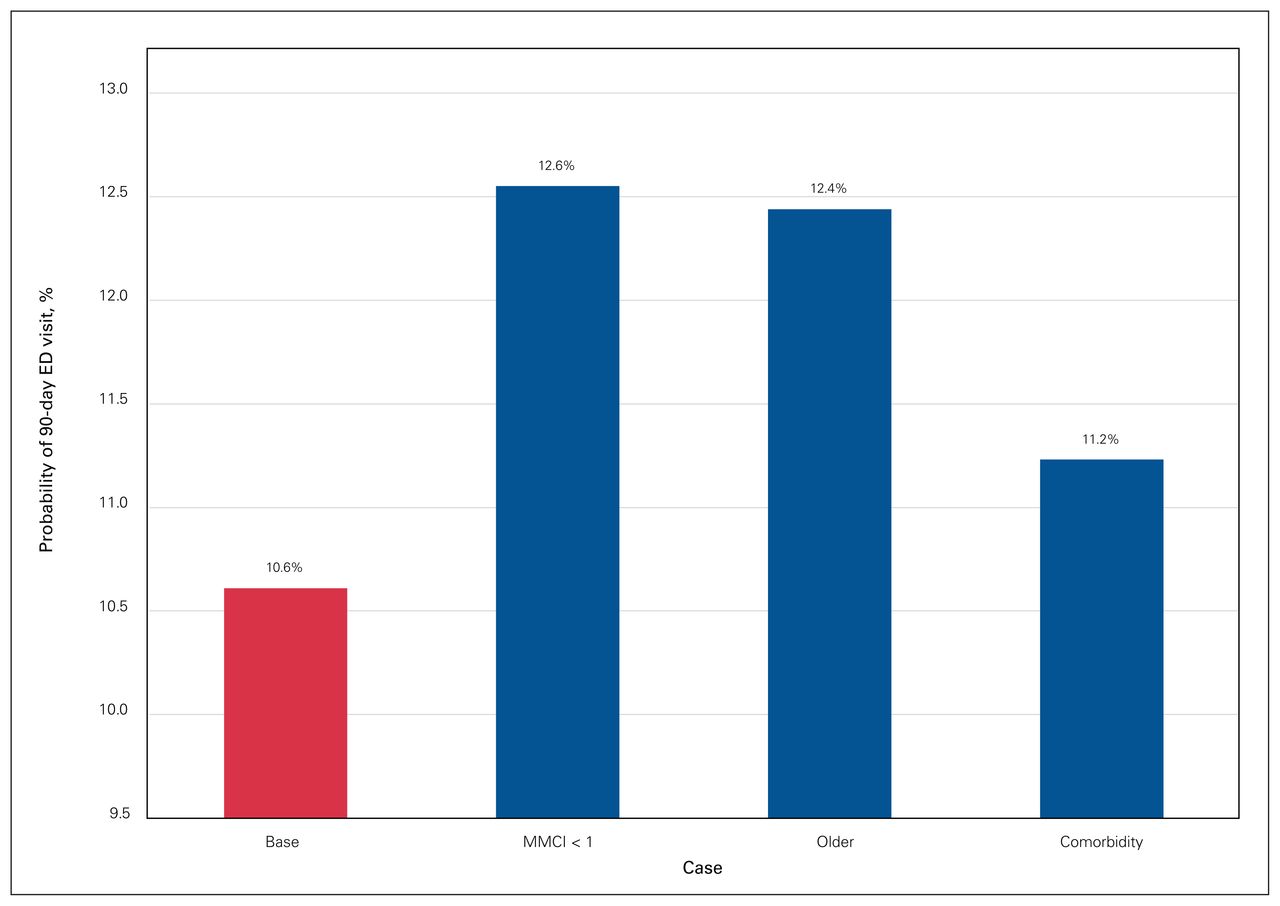
Figure 1 and Figure 2 show the probability of an ED visit for the base case scenario where the MMCI is equal to 1 as well as comparisons to the base case for the case without perfect continuity of care, the older case and the case with a comorbidity. A knee replacement base case with a single primary care provider had a 90-day ED visit probability of 12.8%. If that same individual had multiple primary care providers before surgery, the probability increased to 15.2%. If the base case individual was 10 years older (i.e., changed from age group 60–69 to 70–84 yr), the probability increased to 13.8%, and the presence of a comorbidity increased the probability to 13.6% (Figure 1). For the base case with a hip replacement, the probability of an ED visit increased from 10.6% to 12.6% when multiple primary care providers were seen. A 10-year increase in age increased the probability to 12.4%. There was a smaller increase, to 11.2%, in the presence of a comorbidity (Figure 2).
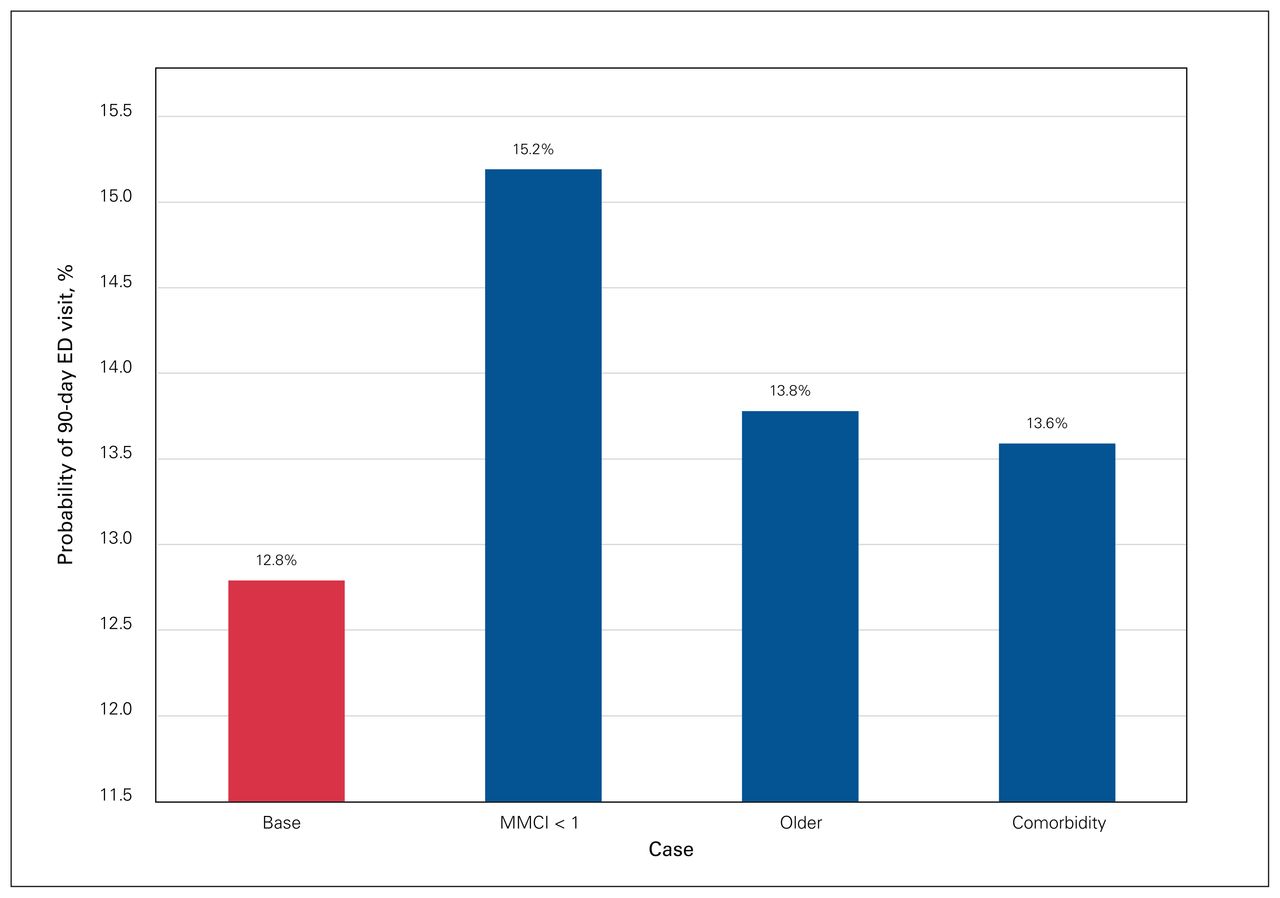
Comparison of predicted probabilities of a visit to the emergency department (ED) within 90 days of knee replacement surgery for the base case, the case without perfect continuity of care (Modified Modified Continuity Index score [MMCI] < 1), the older case and the case with a comorbidity. For the base case, all categorical variables were set at reference categories and continuous variables were set at means.
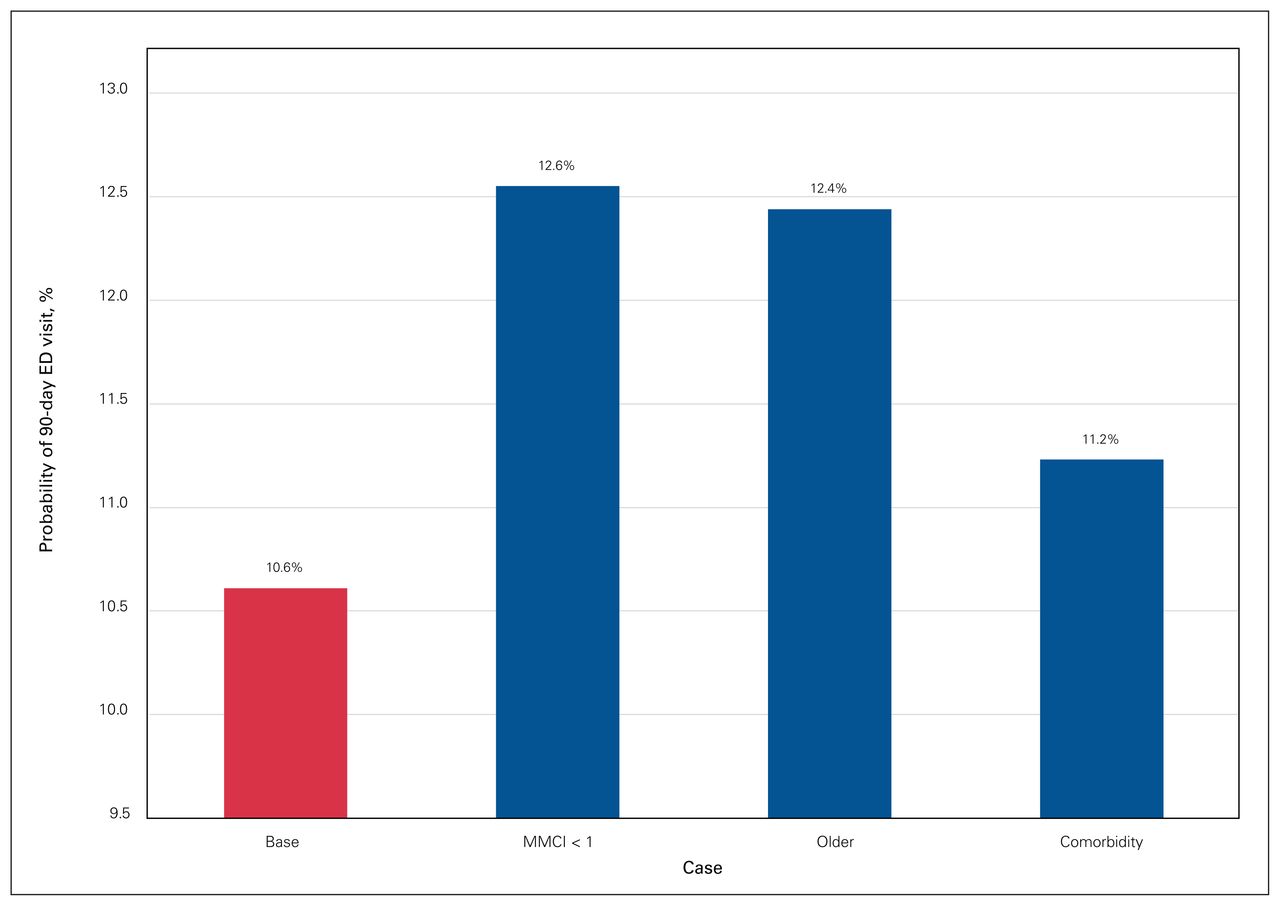
Comparison of predicted probabilities within 90 days of hip replacement surgery for the base case, the case without perfect continuity of care (Modified Modified Continuity Index score [MMCI] < 1), the older case and the case with a comorbidity. For the base case, all categorical variables were set at reference categories and continuous variables were set at means. ED = emergency department.
Discussion
Our study shows that a higher CPC score is associated with a lower probability of a 90-day ED visit after knee and hip replacement. For patients who receive a knee or hip replacement, the effect size of a change from having 1 provider to multiple providers is lower than that for aging by 10 years or having a comorbidity. The results of this study are consistent with previous research showing an association between CPC and ED visits in nonsurgical settings.11–15 Given the projected increase in the rates of joint replacement surgery in the coming decades16,17 and the ensuing strain on health care budgets, these results focusing specifically on joint replacement surgery are highly relevant.
The connection between CPC and ED visits is reflected in the literature both in Canada and internationally.18 Research has demonstrated improved medication compliance, behaviours and patient satisfaction resulting from increased CPC,19 which all have an effect on surgical readiness. The health issues that lead to joint replacement surgery frequently take years to develop with varying degrees of progression, and the management of symptoms can affect preparedness for surgery and subsequently affect postsurgical outcomes.20–24 Furthermore, an initial ED visit after surgery can lead to subsequent visits for patients without access to a primary care provider.25 Primary providers play a key role in managing symptoms and surgical preparation before joint replacement surgery. Greater continuity of care before surgery enables better preparedness, which translates into improved outcomes.
Surgery necessitates transitioning along the continuum of care from primary care to hospital care and back to primary care. As patients progress through the care pathway, coordination of care between primary care providers and surgeons has been shown to improve surgical outcomes.26,27 Despite this, communication between primary care providers and specialists remains a barrier to coordination of care.26,28 Surgeons report having limited time available to contact a patient’s other providers to get a better understanding of their health history.29 It is conceivable that having to communicate with multiple primary care providers would pose further challenges to effective coordination of care.
Results from this study may be helpful in the development of strategies to improve the coordination of care for patients undergoing surgery. Breton and colleagues produced a logic model aimed at improving CPC that includes funding incentives, centralized wait lists and monitoring tools.30 For surgical patients, presurgical checklists have been shown to improve outcomes.31,32 An awareness of the association between CPC and ED visits suggests that surgeons should ask their patients how many primary care providers they have and then use this information to help target those vulnerable to negative outcomes. Furthermore, the use of predictive modelling to estimate the likelihood of negative outcomes including ED visits is becoming increasingly widespread. As suggested by Mahajan and colleagues,33 these models can be continually improved with the inclusion of more risk factors. Knowledge of the link between CPC and ED visits for joint replacement can help in the ongoing development of predictive models.
This study has several strengths. The very large, comprehensive database that we used enabled us to focus precisely on the effect of CPC on ED visits after surgery. Most notably, the inclusion of a covariate indicating a prior ED visit 1 year before surgery controls for unobserved factors that lead to some individuals visiting the ED more frequently. Our results, therefore, better reflect the probability that ED visits were related to patients’ joint replacement surgery and not other factors. Given that the study included data for all of Nova Scotia, a single health administrative jurisdiction, we were able to include ED visits to all hospitals in the province, not just to the facility where the surgery took place. Finally, there is limited research on continuity of care that is not focused solely on primary care.11 By targeting surgical patients, this study adds to the continuity literature.
Limitations
We were unable to identify primary care visits to multiple providers within a single family practice clinic. Care may have been coordinated across providers within a single practice, mitigating the negative effects of having multiple providers. The study did not focus on the specific cause for ED visits. Although an ED visit for any reason is commonly used as a quality indicator after surgery and often reflects appropriateness for surgery, our results could have been strengthened by a comprehensive analysis of the ED visit type.
Conclusion
Our study showed a negative association between CPC and an ED visit within 90 days of hip or knee replacement surgery. Given that the number of these surgeries is expected to increase globally in the coming years, it would be beneficial for health systems to adopt strategies to increase primary care continuity and provide additional support for patients without a regular primary care provider who undergo joint replacement surgery.
Acknowledgement
The data used in this project were made available by the Nova Scotia Department of Health and Wellness (DOHW). Any opinions expressed by the authors do not necessarily reflect the opinion of DOHW.
Footnotes
Competing interests: G. Richardson received travel support from Stryker and DePuy Synthes and has stock or stock options in Stryker. He has also participated in a data safety monitoring board for Hip Innovation Technology. No other competing interests were declared.
Presented at the 2020 Virtual Canadian Orthopaedic Association, Canadian Orthopaedic Research Society and Canadian Orthopaedic Residents Association Annual Meetings, June 19–20, 2020.
Contributors: G. Richardson conceived the study. L. Lethbridge and M. Dunbar analyzed the data. L. Lethbridge wrote the article, which G. Richardson and M. Dunbar critically revised. All authors gave final approval of the version to be published.
- Accepted May 15, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.