


Abstract
Background: Instrumented lumbar surgeries, such as lumbar fusion and lumbar disc replacement, are increasingly being used in the United States for low back pain, with utilization rates approaching those of total joint arthroplasty. It is unknown whether there is a similar pattern in Canada. We sought to determine utilization rates and total medical costs of instrumented lumbar surgeries in a single-payer system and to compare these with the rates and costs of total hip and knee replacements.
Methods: We included Ontarians aged 20 years and older who underwent instrumented lumbar surgery or total knee or total hip replacement between April 1993 and March 2012. Utilization and medical cost of the procedures were evaluated and compared using linear regression in a time-series analysis. Instrumented lumbar surgical procedures were stratified by age and main indication for surgery.
Results: Utilization of instrumented lumbar surgeries rose from 6.2 to 14.2 procedures per 100 000 population between 1993 and 2012 (p < 0.001), well below the utilization of knee and hip arthroplasties. Patients were younger than 50 years for 29.2% of all instrumented lumbar surgery cases; annual procedure rates among those older than 80 years rose 7.6-fold. Direct medical costs of instrumented lumbar surgeries from 2002 to 2012 totaled $176 million. Spinal stenosis and spondylolisthesis were the most common indications for instrumented lumbar surgeries.
Conclusion: Use of instrumented lumbar surgeries in Ontario’s single-payer system has increased rapidly, especially among patients older than 80 years. In contrast to the situation in the United States, these rates were well below those of total joint arthroplasties. These data provide useful insights about resource allocation for surgical treatment of lumbar degenerative disorders.
Chronic back pain is a disabling condition that affects a significant proportion of the general population: epidemiologic surveys suggest two-thirds of Americans have back pain at some point in their lives, while 15% have frequent or prolonged backache.1 The prevalence of back pain is also higher with lower levels of education and income,1 which, combined with the high economic costs of this condition to patients,2 represents a significant burden of illness. Indeed, the Global Burden of Disease study suggests low back pain has risen to become the sixth leading cause of morbidity worldwide, accounting for more than 83 million disability-adjusted life-years lost.3
One of the procedures increasingly employed in chronic back pain management is fusion of the lumbar vertebrae.4–7 Originally devised as a treatment for symptoms of spinal tuberculosis,8 spinal fusions have become widely used for the treatment of fractures, deformity and degenerative conditions of the spine. More recently, artificial lumbar disc replacement was approved by the Food and Drug Administration in the United States for treatment of degenerative disease, expanding the armamentarium of surgical treatment for back pain. In the US, a 6-fold increase in the use of lumbar fusion for the treatment of degenerative lumbar conditions was observed from 1993 to 2011, with an increasing trend of instrumentation that includes insertion of screw-rod constructs and/or interbody cages.5,6 Meanwhile, use of artificial lumbar disc replacement has lagged, accounting for only 2.7% of lumbar degenerative disc disease cases from 2005 to 2009.9 Concomitant with increased utilization, the cost of fusions has risen drastically, reaching a median total hospital charge of over US$30 000 in 2001.5 This trend has translated into a dramatic burden in total spending on fusion surgeries; in the US, $40 billion is spent annually on spinal fusions, more than on any other hospital-based surgery.10
Despite this drastic increase in both rates and cost, evidence is limited for the efficacy and effectiveness of surgery as a treatment for low back pain associated with degenerative disc disease,11–15 the most frequently cited diagnoses for the use of the procedure.7 A 2009 review of evidence for an American Pain Society clinical practice guideline concluded that spinal fusion was no more effective than intensive rehabilitation with cognitive behavioural therapy in the treatment of nonradicular back pain.16 Curiously, rates of spinal fusion in the US now approach those of hip and knee replacements,7,17 2 procedures with a more established evaluation of efficacy.18,19 Currently, there is little information on the trend and cost of instrumented lumbar surgeries (ILS) such as lumbar fusion and lumbar disc replacement in Canada, which has a single-payer health system. Furthermore, it is unclear whether the indications for the procedures in Canada are similar to those observed in the US. In this study, we sought to determine the longitudinal utilization rates associated with ILS in Ontario, Canada’s largest province, with a population of 13.6 million, and to compare these with the rates of total hip and knee replacements to evaluate whether they mirror trends observed in the US. Further, we aimed to evaluate the direct medical costs of, and the main surgical indications for, ILS in Ontario.
Methods
Identification of patients and procedures
Using administrative databases housed at ICES, we identified all patients aged 20 years and older who underwent ILS, total knee arthroplasty or total hip replacement between Apr. 1, 1993, and Mar. 31, 2012. A case of ILS was defined using a modified algorithm of Canadian Classification of Health Interventions (CCI) procedural codes, International Classification of Diseases (ICD) diagnostic codes (see below for details) and Ontario Health Insurance Plan (OHIP) procedural codes (Appendix 1, available at canjsurg.ca/017016-a1).20 Claim codes pertaining to spinal diagnoses have been validated against the gold standard of physician review; interrater κ coefficients for disc herniation, spinal stenosis and acquired spondylolisthesis were 0.88, 0.74 and 0.73, respectively.21 Canadian case definitions of total knee arthroplasty and total hip replacement for this study were established previously (Appendix 1).22 People with fracture, tumour, infection, inflammation or a primary diagnosis of nonlumbar spinal pathology were excluded. In 2002, the diagnostic coding system was changed from the International Classification of Diseases, 9th revision (ICD-9) to the enhanced Canadian version of the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10-CA) system; the Canadian Classification of Diagnostic, Therapeutic and Surgical Procedures (CCP) was changed to the CCI during the same time. Data through Mar. 31, 2002, were coded using the ICD-9/CCP system, and ICD-10CA/CCI codes were used from Apr. 1, 2002, onward.
Data sources
Four databases housed at ICES were linked for this study: the Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD), CIHI’s Same-Day Surgery Database (SDS), the OHIP database and the Registered Persons Database (RPDB). The CIHI-DAD and SDS databases provide data on all visits to acute, rehabilitation, chronic and day surgery institutions in Ontario. The quality of the data in CIHI-DAD was validated through a reabstraction and interrater reliability study in 2002–2004.23 A high level of agreement was found for patient demographic data. For Main Responsible Diagnosis coding, overall agreement was 85% in the reabstraction study and there was a κ score of 0.81 in inter-rater reliability. 23 Of note, orthopedic diagnoses such as hip arthrosis, knee arthrosis and femur fractures have greater than 90% agreement and are among the diagnostic codes with the highest rates of agreement in the study.24 The CIHI-DAD database was also used to calculate resource intensity weight-adjusted inpatient costs associated with the procedure. The OHIP database was used in an algorithm with DAD/SDS to identify eligible cases, as well as physician reimbursement for these procedures. The RPDB contains basic demographic information for everyone to whom an Ontario health card has been issued.
Baseline data
Baseline demographic information (age, sex) was collected. Postal code information was used to assign each patient to their local health integration network. Charlson comorbidity index scores were compiled on the basis of ICD diagnoses in CIHI-DAD. The RPDB was used to identify additional demographic information for the patients, such as their postal code, which served as a proxy for the location of residence. Other demographic information, such as urban/rural status, was obtained from the Canadian census on the basis of postal codes.
Statistical analysis
The annual rates of ILS, total knee arthroplasty and total hip replacement were determined relative to the population. Linear regression was used to determine trends in surgical rates in a time-series analysis. In addition, age-standardized analysis was carried out to account for demographic changes over the span of cohort accrual during the time period of the study. ILS rates were further subdivided into their components and stratified by the indications for which they were performed. Annual procedural costs, presented in 2011 Canadian dollars, were adjusted for inflation using the Bank of Canada’s inflation calculator (http://www.bankofcanada.ca/rates/related/inflation-calculator/). Procedural costs of the 3 procedures were derived using the resource intensity weight method via the %getcost macro developed by ICES to provide person-level costing in Ontario.24 CIHI-DAD classifies all acute discharges by case mix groups; this classification system was developed to categorize groups of patients with similar clinical and resource utilization patterns. Standardized inpatient costs within a case mix group are then adjusted by the resource intensity weight, an indicator representing the level of resources used relative to a reference case (cost per standardized case × resource intensity weight), to estimate the specific case cost of a given hospital admission.24 The %getcost macro draws upon databases pertaining to inpatient hospital admissions, emergency and ambulatory visits, same-day surgeries, inpatient rehabilitation, home care and physician services to generate case costs associated with each health care encounter.24 In the inpatient setting, these costs primarily involve acute inpatient utilization and physician services. Socioeconomic status was calculated through income quintiles using postal codes and income information available from dissemination areas of the Canadian census data available from Statistics Canada. Geographic location and rurality were determined via Statistical Area Classification (SAC) codes available from Statistics Canada. The Charlson Comorbidity Index was used to account for comorbidity. A p value of 0.05 was used to define a statistically significant difference. All analyses were done using SAS statistical software.
Ethics
The study was approved by the Health Sciences and Affiliated Teaching Hospitals Research Ethics Board at Queen’s University.
Results
Over the study period, 16 363 ILS procedures were performed in Ontario; by comparison, 233 281 knee arthroplasties and 154 381 total hip replacements were completed over the same period. Patients undergoing lumbar procedures were younger, had lower comorbidity and were more likely to have undergone the procedure at a large teaching hospital than patients undergoing the other 2 types of procedures (Table 1). The majority of the procedures were completed by orthopedic surgeons.
Baseline clinical and utilization characteristics
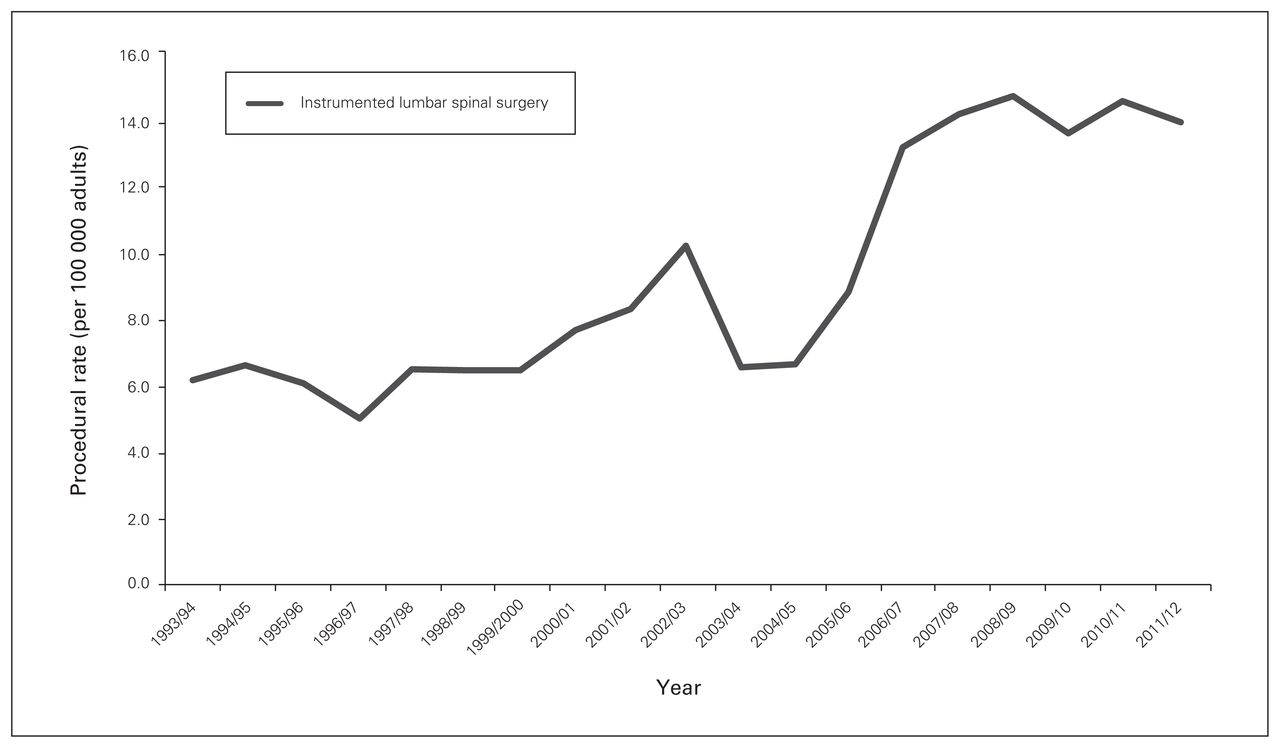
Utilization of ILS rose from 6.2 to 14.2 procedures per 100 000 population between 1993 and 2012 (p < 0.001) (Fig. 1); this was maintained with age standardization to account for demographic changes over time. These rates were well below the rates of knee and total hip arthroplasty procedures (knee: 64.9–197.4 cases per 100 000; hip: 65.2–111.6 cases per 100 000, p < 0.001 for comparison) (Fig. 2). Patients aged 60–69 years were the highest users of ILS (24.3% of all cases) among age deciles, followed by those aged 70–79 years (21.6%). Meanwhile, 29.2% of all cases involved patients younger than 50 years. The number of procedures completed on patients 80 years of age and older rose from 13 in 1993 to 99 in 2012.

Rates of instrumented lumbar spinal surgery in Ontario per 100 000 adults.

Rates of total knee replacement, total hip replacement and instrumented lumbar spinal surgery in Ontario per 100 000 adults.
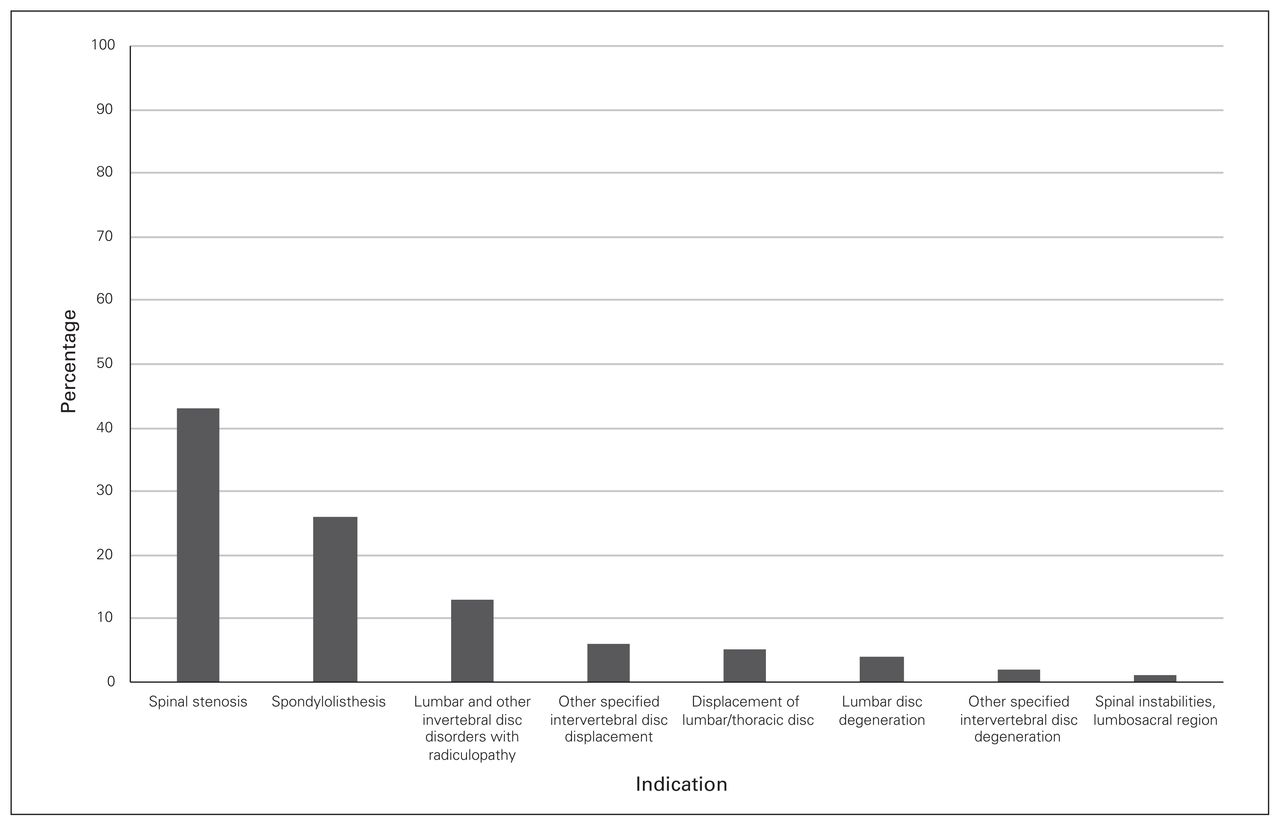
Lumbar stenosis and spondylolisthesis were the most common main diagnoses among the lumbar surgical interventions performed, accounting for 69% of the procedures. Lumbar disc degeneration was the diagnosis for only 4% of procedures (Fig. 3).

Distribution of indications involving instrumental lumbar surgical procedures in Ontario.
Length of hospital admission for ILS steadily declined from 8 to 4 days and from 8 to 5 days for men and women, respectively, over the study period. There was little difference across provider type, hospital type (teaching v. nonteaching) or geographic location. Stratification by age revealed the largest reduction in length of stay among patients aged 80–89 years, from 17 days in 1993 to 5 days in 2012, followed by patients aged 70–79 years, for whom length of stay fell from 11 days to 5 days (Table 2).
Median length of stay (in days) for lumbar surgery stratified by age group
The direct medical cost of the 2 lumbar interventions rose from $13 million in 2002 to $24 million in 2012; overall, $176 million in medical costs accrued during this period (Table 3).
Direct medical cost of lumbar surgery between 2002 and 2011
Discussion
In this population-based study of surgical interventions for degenerative lumbar conditions, we found moderate increases in ILS rates, with the highest growth among patients aged 80 years and older. The overall utilization, of ILS, however, was well below the utilization of knee and total hip arthroplasty.
The rates of ILS utilization were markedly lower in this study than those reported in a similar population-based US study. Rajaee and colleagues reported that annual rates of lumbar fusion increased from 64.5 to 135.5 per 100 000 adults from 1998 to 2008, an increase approximately 10-fold higher in absolute terms than reported here.7 Our finding is consistent with work by Lavis and colleagues, who noted a 3.4-fold higher rate of spinal fusion for mechanical neck and back pain in the US compared with Ontario.25 Our lumbar surgery rate estimates are slightly lower than those reported in a 2009 study using similar databases, which demonstrated a 40% increase in the rate of procedures between 1995 and 2001 in Ontario.26 This was probably because Bederman and colleagues’ cohort was restricted to people under the age of 50 years, resulting in an enriched population with a higher prevalence of lumbar surgery.
Although rates of spinal fusion in the US now approach those of hip and knee replacement,7,17 similar trends were not seen in Ontario, where ratios of ILS to hip and knee replacements were approximately 1:8 and 1:14, respectively. Several health system and policy factors probably contributed to this divergence, especially resource allocation decisions in Canada’s single-payer system. In response to the 2003 First Ministers’ Accord on Health Care Renewal and the 10-Year Plan to Strengthen Health Care signed during the following year, $5.5 billion was allocated over 10 years to reduce wait times in Canada.27 Strategic priority was given to 5 clinical areas, 1 of which was hip and knee arthroplasties. In a setting where hospitals receive global operating room budgets, it is expected that targeted orthopedic procedures would receive higher utilization at the expense of alternative surgeries. It is important to note, however, that the level of evidence associated with the effectiveness of joint replacement is much stronger than that associated with spinal fusions: for example, 2 randomized controlled trials of unilateral total knee replacement among patients with moderate to severe osteoarthritis demonstrated markedly improved pain relief and functional improvement at 12 months.28,29 The role of spinal fusion for low back pain associated with spinal stenosis or spondylolisthesis remains uncertain, especially in the context of recent trials.30 Publication of the Swedish Spinal Stenosis Study demonstrated no clinical benefit associated with adjunctive fusion in addition to decompression for spinal stenosis with or without spondylolisthesis.31 Similarly, the Greenwich Lumbar Stenosis SLIP trial, performed among patients with stable spondylolisthesis, demonstrated potentially more favourable value with decompression alone given the costs of instrumented fusion, and the inability of moderate gains in general quality- of-life outcome to translate to improvement in disease-specific measures.32 The impact of these 2 recent trials on changes in fusion surgery trends would be crucial to reconcile with data from the earlier Spine Patient Outcomes Research Trial (SPORT),33 to ensure that the knowledge gained from these pragmatic comparative effectiveness trials is translated and disseminated in routine care. A recent Ontario comparative outcome and cost-utility study with a retrospective cohort design compared focal lumbar spinal stenosis surgery to total hip and knee arthroplaties and found that the 3 types of procedures offered durable and favourable cost-utility ratios. Similar evaluations of these health technologies in the real-world context, using methodologies to account for residual confounding, are needed to expand the evidence base for ILS in settings other than randomized controlled trials.37
Additionally, we found that close to 1 in 3 patients who received ILS in Ontario were younger than 50 years, and the annual rate of procedures for those aged 80 years and older grew close to 8-fold. The increasing utilization of spinal fusion in the very elderly mirrors trends observed in the US, where age-adjusted rates of fusion increased from 40 to 102 procedures per 100 000 persons.34 Although the rate of adverse events of lumbar fusion among the very elderly was noted to be low, in-hospital mortality was nonetheless higher in this age group than in patients aged 65–79 years.34 Furthermore, this group was poorly represented in the clinical trials in which the efficacy of lumbar fusion was evaluated.31–33
The major strength of our study is its extended time-frame spanning nearly 2 decades, which provides important longitudinal context and secular trends by which to evaluate more recent changes in the case mix of spinal surgical interventions. In addition, our use of administrative data in a jurisdiction with universal medical coverage captures comprehensive, population-based trends. Meanwhile, the high quality of these routinely audited databases, with codes previously validated in the spine population,26 provides confidence about the robustness of our findings.
Limitations
Several limitations need to be acknowledged. First, it is recognized that several methods of case-costing exist, including direct use of data from the Ontario Case Costing Initiative (OCCI), which are used to generate standardized per-case cost in the province. However, OCCI costs are not recorded for all hospitals, and the %getcost macro was used to encompass all hospitals performing ILS in the province. Second, outcomes of ILS were outside the scope of this study, including postsurgical opioid use. Although reductions in opioid analgesic use have been used in randomized controlled trials of spinal devices to assess clinical outcomes,35,36 there has been no efficacy evaluation of spinal fusion surgery at the population-level using administrative medication databases, an important area of exploration. Third, although surgical indications for ILS procedures, including spondiloliesthsis and lumbar stenosis, are generally associated with radicular pain, the nature of administrative databases precluded confirmation of symptoms in the preoperative setting. Similarly, the database we used is unable to definitively separate isthmic and degenerative spondylolisthesis, despite patients with fractures having been excluded from our study. Finally, administrative data are inherently susceptible to miscoding, and errors between interbody fusion and lumbar disc replacement remain possible given the novelty of the latter procedure. Therefore, rates of fusion and lumbar disc replacement were not separately analyzed; rather, these 2 types of procedures were unified as instrumental lumbar surgeries.
Conclusion
In a population-based cohort spanning 19 years, there was a modest increase in utilization of ILS among Ontario adults. Use of these lumbar procedures has grown rapidly among the very elderly, a group poorly represented in the randomized trials in which the efficacy of the procedures was rigorously evaluated. In contrast to US trends, however, utilization was well below that observed for joint arthroplasties. The observed decline in length of stay associated with ILS was offset by increased utilization that contributed to the rise in overall direct medical costs for these procedures. Given our finding of increasing utilization of and spending for ILS in Ontario, research aimed at determining both the clinical effectiveness and the cost-effectiveness of these procedures in the long-term, real-world setting35 using patient-oriented outcomes is urgently needed to form an evidence base to inform practice and policy.
Footnotes
Competing interests: None declared.
Contributors: Y. Xu, D. Yen and A. Johnson designed the study. Y. Xu, M. Whitehead, J. Xu and A. Johnson acquired the data, which Y. Xu, D. Yen, J. Xu and A. Johnson analyzed. Y. Xu wrote the article, which all authors reviewed and approved for publication. All authors agreed to be accountable for all aspects of the work.
- Accepted January 24, 2019.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.