


Summary
Oncoplastic breast surgery combines certain plastic surgery procedures with a breast cancer resection to minimize the cosmetic penalty. We compared current practices in breast surgery in Canada and the UK, looking at the classification of oncoplastic breast surgery, management of larger tumours that would otherwise mandate a mastectomy, and the breast surgeon’s role in immediate breast reconstruction. Reconstructive breast surgery has always fallen within the domain of the plastic surgeon, but surgical subspecialization and more focused fellowship training have meant that breast surgeons with the appropriate skillset can offer these procedures. This evolution of the breast surgeon has led to the birth of a new field of breast surgery known as oncoplastic and reconstructive breast surgery. Those tasked with developing surgical training programs in Canada must now decide whether to train breast surgeons in these techniques to improve long-term quality of life among Canadian patients with breast cancer.
Overall survival for patients with breast cancer is now better than ever.1 Advances in adjuvant treatments have also resulted in better disease-free survival. Furthermore, long-term follow-up data spanning 20 years now give definitive support to the equivalent survival outcomes of breast conservation surgery compared with mastectomy.2,3 Given the equivalence in mortality between these surgical options, patients are now offered a choice between the two types of surgery. Data suggesting an inferior psychosocial outcome (including increasingly negative body-image issues) in women undergoing mastectomy also fuel the argument to reduce mastectomy rates at a unit level, provincially and, ultimately, nationally.4,5
As a result of this improved survival, physicians treating breast cancer must now consider a new concept known as survivorship. Although relevant at a multidisciplinary and holistic level, surgeons can contribute immensely to the effects of treatment by giving thought to their patients’ long-term physical and psychosocial outcomes after their index operation. Fifty years ago, when the prognosis of breast cancer was dismal, breast surgeons would seldom give much thought to such matters as sympathetic scar placement during breast conservation surgery; leaving an esthetically pleasing mastectomy scar (such that patients are not left with excess skin over the chest wall or in the axilla and that they have as much upper-pole skin retained as possible for future possible delayed flap-based reconstruction); the option of breast conservation surgery; or immediate breast reconstruction. In fact, the decision to perform a mastectomy was left to the surgeon’s discretion, and women were unaware of whether they had received a mastectomy or not until they awoke from general anesthetic.
Increased patient awareness as well as a greater degree of transparency from the medical profession has meant that standards of care such as these are no longer acceptable to the general public. Not only are physicians more accountable, but — with the Internet revolution — patients are better informed and have more confidence to question the care they receive.
Oncoplastic and reconstructive breast surgery was born out of a need to address the issue of longer-term patient-reported outcomes after surgery while still maintaining steadfast oncological principles. Although safe and adequate tumour resection will always be of primary importance to breast surgical oncologists, we are now being asked to leave patients with better esthetic outcomes that will not stigmatize them in the future. As patients are living far longer after completing their breast cancer treatment, they do not want their scars and their reflection in the mirror to serve as a daily reminder of their breast cancer diagnosis.
Definition
When defining oncoplastic and reconstructive breast surgery, Clough and colleagues6 proposed a bi-level classification depending on the volume of breast tissue excised and the amount of glandular reshaping and nipple repositioning required (Table 1).
Oncoplastic decision guide
This concept was expanded by a multidisciplinary panel convened by Lebovic in 2010 at the American Society of Breast Disease Annual Symposium to four levels depending on skill and competence. The general surgery curriculum in the UK now asks that British general surgery trainees who plan to be breast surgeons must meet a number of essential competencies, some of which have historically been found within the plastic surgery syllabus. Every new breast surgeon in the UK must demonstrate the ability to perform both level 1 and level 2 oncoplastic breast conservation (e.g., therapeutic reduction mammoplasty — a breast reduction excising the tumour with a margin) as well as immediate breast reconstruction in the form of implant-only or pedicled myocutaneous latissimus dorsi flaps. Breast surgeons are also trained in fat grafting — using fat removed by liposuction from the abdomen and thighs to correct deformities left after breast conservation surgery and to improve final results after breast reconstruction. Free-flap reconstruction, as a result of the need for microvascular skills, remains firmly in the domain of the plastic surgeon.7 The logical outcome of producing more surgeons skilled in oncoplastic breast conservation and immediate breast reconstruction are a reduction of the overall mastectomy rate (as larger tumours can be resected using partial breast reconstruction techniques) and an increase of the rate of immediate total breast reconstruction. Furthermore, longer-term patient-reported outcome measures in emotional, physical and sexual domains improve.8
Existing training opportunities
It is widely accepted that North America has lagged behind Europe not only in adopting oncoplastic breast surgery, but also in training its breast surgeons to perform breast reconstruction. Perceived barriers to this practice have previously been described in the literature,9 but the reasons for a lack of breast surgeons who are trained in breast reconstruction are multifactorial.
A handful of specific breast surgical oncology fellowships do exist in Canada, and an impressive fellowship program is offered by Western University. Two separate publications have not only described the current fellow’s logbook, demonstrating a wide range of oncoplastic and reconstructive surgical procedures, but also summarized oncoplastic training opportunities in Canada.10,11 The University of Ottawa offers a dedicated oncoplastic and research fellowship that includes exposure to breast reconstruction. The University of Toronto breast surgical oncology fellowship offers a one-year breast surgical oncology program that includes exposure to oncoplastic surgery. Similarly, Western University also offers a one-year breast fellowship that includes training in oncoplastic surgery. The oncoplastic partnership workshop is a cadaveric workshop that takes place every few months and is open to breast surgeons with a surgical volume of more than 20 cases per year. This innovative and unique workshop, which is organized in Toronto, Ottawa and London, Ont., includes a hands-on session as well as didactic teaching on all aspects of oncoplastic breast surgery and nipple-sparing mastectomy.
The UK training interface group (TIG) in oncoplastic breast surgery is an example of a program that draws applicants from both general surgery and plastic surgery backgrounds to the same national training program. The training syllabus not only includes oncoplastic breast conservation surgery, as is taught in the Canadian fellowships and workshops, but also includes implant-based and autologous total breast reconstruction. Twelve fellowship-trained breast surgeons competent in both the resectional and reconstructive components of breast surgery have been produced every year since the TIG’s inception in 2002 — a phenomenal achievement given that other parts of the developed world produce almost none.
Onoplastic breast conservation — technical considerations
Level 1 oncoplastic breast surgery is within the skillset of any breast surgeon. Sympathetic scar placement (either in the periareolar, inframammary or lateral breast fold regions) results in esthetically pleasing scars.16 Incisions placed in the upper pole of the breast (especially those placed above the bra line) should be used only in exceptional circumstances. Once a full-thickness resection from subcutaneous fat to pectoralis fascia has been performed, even minor glandular mobilization can minimize any divot left behind. This basic form of volume displacement surgery can have very satisfactory results. This concept can be extended to the so-called modified Benelli round-block technique (also known as a donut mastopexy). During this procedure, a narrow 2 mm rim of skin is de-epithelialized around the nipple-areolar complex. The index quadrant containing the tumour is dissected in the oncological plane between subcutaneous fat and breast parenchyma. Once this dissection has been taken past the tumour, it is widely excised — as in any segmental resection — down to pectoralis fascia. Once the specimen has been removed and the cavity marked with radio-opaque clips, dual-plane mobilization between retromammary fascia and pectoralis fascia as well as the subcutaneous fat/breast parenchyma plane is performed. This dissection raises two symmetric parenchymal flaps that can then be apposed with loose sutures in order to close the defect left behind from the tumour resection. Patients are generally warned that their breast volume will be smaller (perhaps a cup size smaller) and of the possibility of fat necrosis and the resulting lumpiness.
Level 2 oncoplastic breast conservation is used when 20%–50% of breast volume is to be excised. This usually requires more specialist training, as it involves raising the nipple on a pedicle and extensive glandular mobilization together with skin undermining in order to “re-drape” the breast skin over the breast mound in a tightening manoeuvre. Numerous techniques can be used; one of the most common is the Wise pattern incision, raising the nipple on either an inferior, superomedial or superior pedicle. These complex incisions carry a higher risk of wound breakdown, especially in higher-risk groups such as smokers, patients with a high body mass index and patients with diabetes (Fig. 1).

Patient with grade 3 ptosis who initially underwent conventional segmental resection for left breast upper pole multifocal carcinoma with positive margins (upper pictures), who then underwent nipple-sacrificing therapeutic reduction mammoplasty with contralateral symmetrising mammoplasty to successfully achieve clear margins, maintain symmetry and be left with a more manageable breast shape (lower pictures).
Level 2 oncoplastic breast surgery can also be used for central/retroareolar tumours. Conventionally, these tumours would be managed with a central excision, leaving the patient with a transverse scar in place of the nipple-areolar complex. Alternatively, a Grisotti flap can be used to create a neoareola. The tumour is excised via a circular periareolar incision, taking the dissection down to the pectoralis fascia. Preoperatively, a circle with a similar diameter to the areola is marked immediately inferolaterally to the nipple. This neoareola is then advanced as a rotational flap into the defect left behind by the tumour resection. This option is best suited to women with a reasonable breast volume who would like to retain a circular areola onto which a nipple may or may not be reconstructed (or tattooed) in the future, depending on the patient’s wishes.
“Extreme” oncoplastics
It is widely accepted that patients undergoing a mastectomy with immediate reconstruction followed by post-mastectomy radiotherapy can have the worst cosmetic outcomes of all — especially when an implant is involved — owing to the resulting risk of capsular contracture.
The reasons to recommend mastectomy include a large tumour:total breast volume ratio, a history of prior breast radiotherapy, multicentricity, pregnancy (precluding the option of breast radiotherapy) and patient preference. The dogma that tumours larger than 5 cm must be managed with a mastectomy is now largely outdated. More and more patients may undergo conservation surgery knowing that there is a body of evidence confirming the safety of their decision.
Silverstein and colleagues17 were the first to introduce the idea of large tumour resections during oncoplastic breast conservation. They therefore defined this “extreme” group as patients undergoing breast conservation who would otherwise not only have been advised to undergo a mastectomy, but also may have needed post-mastectomy radiotherapy (e.g., patients with tumours > 5 cm, multifocal tumours, multicentric tumours and those with positive lymph nodes). After a median follow-up of 24 months, Silverstein and colleagues17 reported a 1.4% local recurrence rate (LRR). Their results were confirmed by Fiddes and colleagues18 in a slightly larger study population. After a median follow-up of 64 months, the local recurrence rate was 2.7% (well within the expected < 3% LRR at 5 yr).
A recent analysis of the Surveillance, Epidemiology and End Results (SEER) 18 registry looking specifically at triple negative breast cancer (TNBC) shows an improved breast cancer–specific survival (BCSS) and overall survival (OS) with breast conservation surgery and radiotherapy compared with mastectomy.19 Furthermore, when looking specifically at 164 patients with TNBC larger than 5 cm, a superior survival was seen in the breast conservation surgery and radiotherapy group than in the mastectomy group. There is therefore an increasing level of evidence in the literature supporting oncoplastic breast surgery for tumours larger than 5 cm, as long as the basic oncological principle of a clear margin is maintained.
Immediate breast reconstruction
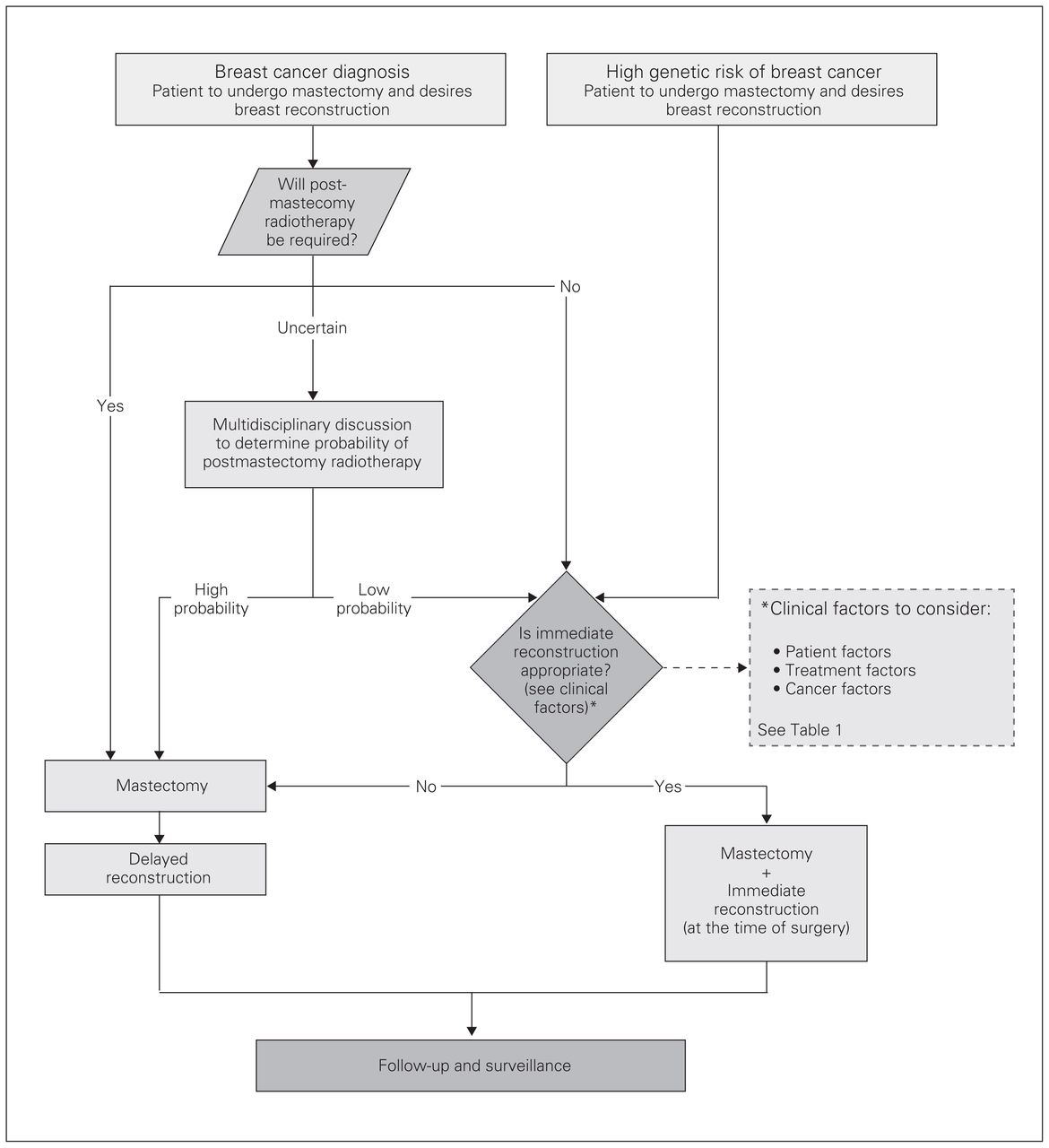
Provincial guidelines state that when counselling patients with primary breast carcinoma regarding a mastectomy, the treating surgeon should mention the option of immediate breast reconstruction.20 Furthermore, information regarding this option should be made available early in the decision-making process. Clearly, some patients will not be suitable for immediate breast reconstruction based on tumour factors (e.g., need for post-mastectomy radiotherapy) and patient factors (e.g., significant comorbidities). Provincial guidelines on breast reconstruction exist, and clinicians are encouraged to use an algorithm in order to determine the timing of referral for breast reconstruction (Fig. 2).

Algorithm for the use of breast reconstruction in patients undergoing mastectomy.20
Anxiety, depression and poor body image have all been reported in patients undergoing mastectomy, and breast reconstruction can alleviate some of this distress. For this reason, the direction of breast surgery seems to be heading toward not only reducing mastectomy rates, but also increasing immediate breast reconstruction rates. The UK National Mastectomy and Reconstruction Audit published four annual reports, the last in 2011.8 This national snapshot of reconstructive practices in the UK suggested an immediate breast reconstruction rate of 21%. There are no contemporary data confirming the current rate of immediate breast reconstruction in Canada, but studies have suggested rates as low as 7%, and regional studies report rates varying between 4% and 14%.21–23
A lack of plastic surgeons specializing in breast reconstruction is often cited as the main reason for low rates of immediate breast reconstruction in Canada. It therefore stands to reason that increasing the number of surgeons performing immediate breast reconstruction will increase rates. Surgical training in Europe has evolved immensely over the past few decades, with immediate breast reconstruction now a mandatory competency for any British breast surgery trainee. Therefore, every breast surgeon qualifying in the UK will be able to perform immediate breast reconstruction in the form of implant-based reconstruction and pedicled latissimus dorsi breast reconstruction with or without an implant (Fig. 3). It is this evolution of the breast surgeon that has led to rising rates of immediate breast reconstruction.

Patient with right upper pole breast carcinoma (preoperative photos above) who opted for a right nipple-sparing mastectomy and sentinel node biopsy with immediate acellular dermal matrix-assisted subpectoral implant reconstruction (postoperative photos below; one-stage, single-surgeon).
To adopt a policy like this in Canada will take decades. Not only will we need multiple nationwide centres offering general surgery residents with an interest in breast surgery the chance to work with a breast surgeon offering immediate breast reconstruction, but also the Canadian general surgery curriculum will have to evolve to reflect this change. The first step down this long road will no doubt be employing more breast surgeons who can perform immediate breast reconstruction in Canadian hospitals. Masterclasses and workshops have been immensely successful in other parts of the world in enabling such surgeons to demonstrate various oncoplastic and reconstructive techniques to other breast surgeons who wish to adopt this practice. As in Edmonton, it takes a few forward-thinking breast surgeons who want to effect change to take this first step.
Conclusion
There is a great opportunity for breast surgery in Canada to evolve. Modern practices in oncoplastic breast conservation as well as selected forms of immediate breast reconstruction after mastectomy should fall within the repertoire of the breast surgeon. Adequate training opportunities for our residents in this type of surgery are paramount in ensuring that the momentum for this change continues and that oncoplastic breast surgery becomes the standard of care in Canada. Employing more oncoplastic-trained breast surgeons who perform select immediate breast reconstruction is the first step toward improving options and, ultimately, quality of life for our patients with breast cancer.
Footnotes
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
- Accepted January 30, 2018.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.