


Summary
The Sainte-Justine Head Trauma Pathway helps physicians’ decision-making in the evaluation of head trauma in young children. We evaluated the pathway to identify clinically important traumatic brain injury (ciTBI) among children younger than two years who presented to a pediatric emergency department for a head trauma. The primary outcome was ciTBI, defined as a TBI complicated by death, neurosurgery, intubation or hospitalization for more than one night. Among 2258 children, we reviewed the charts of all hospitalized children (n = 100) and a random sample of nonhospitalized children (n = 101) and found a ciTBI in 26 patients. The Sainte-Justine Head Trauma Pathway and the Pediatric Emergency Care Applied Research Network Pediatric Head Injury Prediction Rule both had a sensitivity of 96% (95% confidence interval 81%–100%). We found that the Sainte-Justine Head Trauma Pathway does not improve the identification of ciTBI among young children with head trauma.
Head trauma is a common chief complaint among children visiting the emergency department (ED). The Pediatric Emergency Care Applied Research Network (PECARN) Head Injury Prediction Rule is the decision tool currently used in many institutions.1 Its main limitation is that 33% of children younger than two years fall in the moderate-risk category, which entails the physician selecting further investigations based on various factors.1 Identification of a skull fracture would modify the management decisions of approximately half of Canadian pediatric emergency physicians.2 In 2015, a new clinical decision rule was reported to identify children at risk of skull fracture following head trauma: the C-3PO rule.3 Merging the C-3PO rule with the PECARN rule might facilitate the management of traumatic brain injury (TBI) in all children younger than two years while minimizing the limitations of each individual rule. With this aim in mind, the Sainte-Justine Head Trauma Pathway was proposed. Following its development, we aimed to measure the impact of the pathway in identifying children with clinically important TBI (ciTBI).
We conducted a retrospective study of all children younger than two years with a chief complaint of head trauma visiting our university-affiliated pediatric hospital between 2013 and 2015. Children were dichotomized in two groups: all hospitalized children and a 5% random selection of all nonhospitalized children. We reviewed the complete medical chart of each eligible participant. Information was collected by a single coauthor (S.S.) using the standardized case report form, while a second coauthor (J.G.) evaluated a random sample of 5% of health records to assess data accuracy. We measured the interrater reliability using a κ score. The primary outcome was the presence of a ciTBI, defined as a TBI complicated by death, neurosurgery, intubation of more than 24 hours or hospitalization for more than one night.1
Our primary analysis sought to determine the proportion of children with ciTBI that would have been accurately identified using the Sainte-Justine Head Trauma Pathway and the PECARN rule.1 For this analysis, participants were distributed in high-, moderate- and low-risk categories according to their baseline characteristics and radiological investigations. In a secondary analysis, results were extrapolated to the full population of all eligible children. We included all children admitted to hospital with a chief complaint of head trauma in order to include all cases of ciTBI. This was expected to yield a sample of approximately 100 children and at least 20 children with a ciTBI. It was estimated that a random sample of 5% of nonhospitalized patients would need to be recruited to have at least 100 nonhospitalized patients.
Our institutional review board approved the study, and we obtained a waiver of consent from the patients or their guardians for this project.
Results
During the study period, a total of 2258 children were eligible, including 101 children admitted to hospital. Table 1 shows baseline characteristics of participants. Among them, a ciTBI was reported in 26 participants. All children were hospitalized for more than 24 hours, three had a neurosurgical intervention (including one who was intubated for more than 24 hours), and an additional three were intubated for more than 24 hours.
Baseline characteristics of study participants
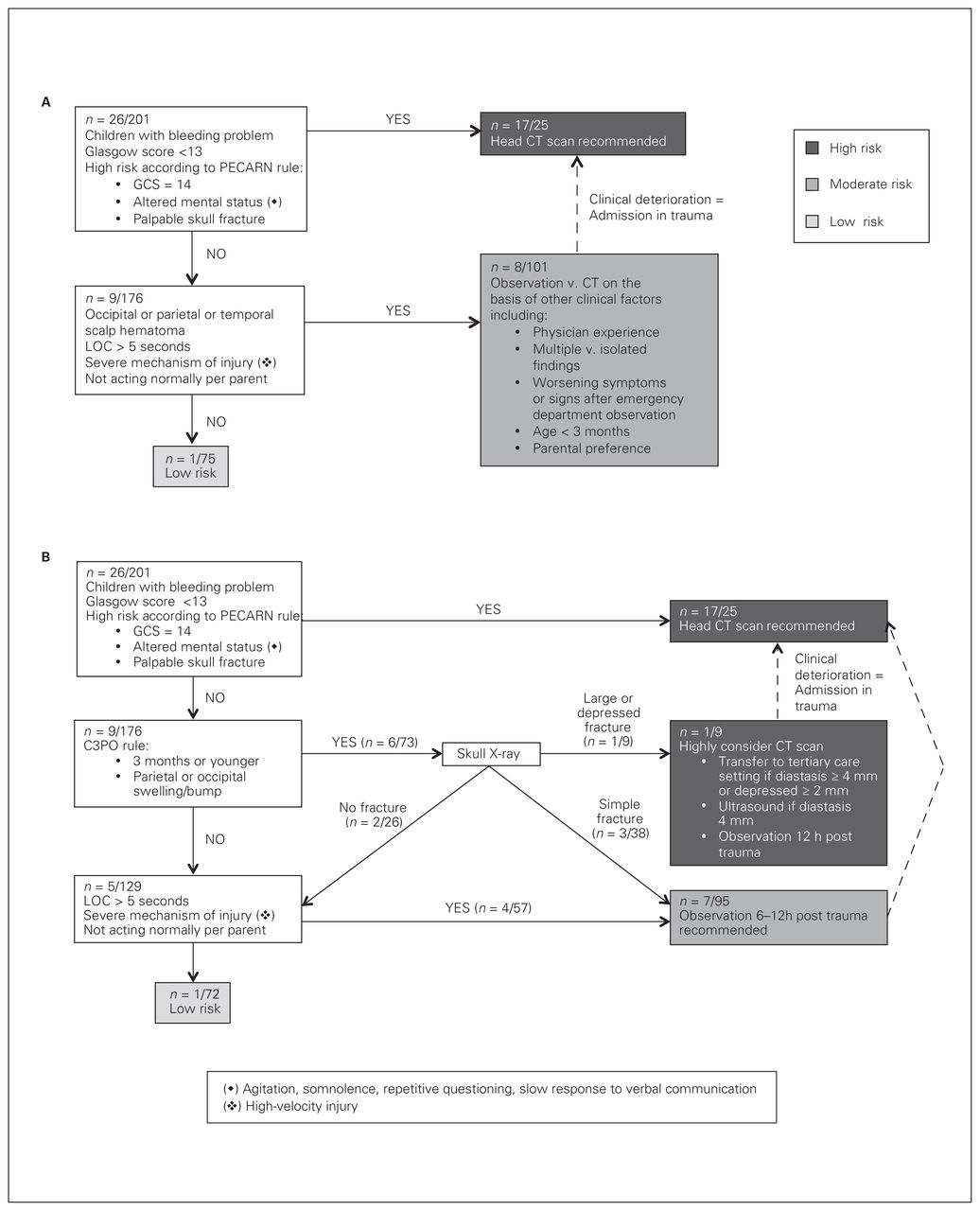
Figure 1 shows the distribution of the 201 participants according to the pathway and the PECARN rule alone. Both strategies showed a sensitivity of 96% (95% confidence interval 81%–100%) and specificities of approximately 41% (Table 2). Applying the distribution to the entire population would yield a rate of ciTBI in each risk category using the clinical pathway: approximately 33% in the high-risk category, 1% in the moderate-risk category and < 0.1% in the low-risk category for both the Sainte-Justine pathway and the PECARN rule (Figure 2).
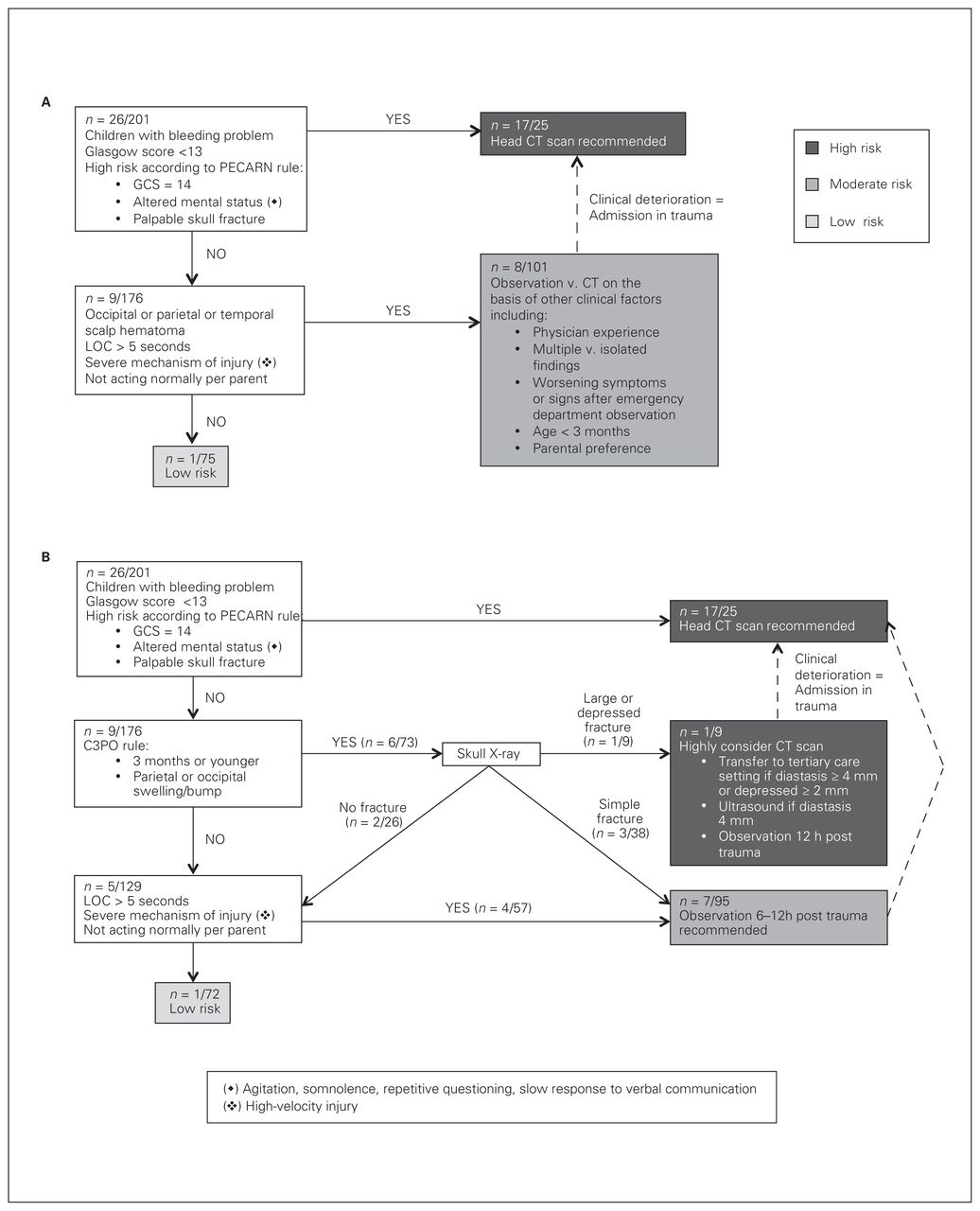
Distribution of the 201 participants according to (A) the Sainte-Justine Head Trauma Pathway and to (B) the Pediatric Emergency Care Applied Research Network (PECARN) Head Injury Prediction Rule. The numerators refer to the number of clinically important traumatic brain injuries (ciTBI). CT = computed tomography; GCS = Glasgow Coma Scale; LOC = loss of consciousness.

Distribution of the full population (extrapolated) according to (A) the Sainte-Justine Head Trauma Pathway and to (B) the Pediatric Emergency Care Applied Research Network (PECARN) Head Injury Prediction Rule. The numerators refer to the number of clinically important traumatic brain injuries (ciTBI). CT = computed tomography; GCS = Glasgow Coma Scale; LOC = loss of consciousness.
Accuracy in identification of patients using Sainte-Justine Pathway and PECARN rule
We evaluated 10 charts in duplicate to assess interrater reliability on the 10 baseline characteristics and items of the pathway. Among them, a perfect agreement was met for five characteristics. An intraclass correlation coefficient (ICC) between 80% and 99% was met for three characteristics, and an ICC less than 50% was calculated for two characteristics (“not acting normally” and “high velocity”).
Discussion
The Sainte-Justine Head Trauma Pathway allowed identification of more skull fractures than the PECARN rule, but it did not improve identification of ciTBI among young children.
Local modifications to the PECARN rule have been suggested in various settings to ease adherence and satisfaction among physicians4 or to improve diagnostic capacity.5,6 The Sainte-Justine pathway was designed to help emergency physicians to stratify the risk among children at moderate risk for ciTBI according to the PECARN rule. Even if more than 33% of our sample still falls in the moderate-risk category, the inclusion of the C-3PO rule allows a better identification of skull fracture, which could improve ciTBI diagnosis. To our knowledge, our study was the first to integrate skull radiography with the PECARN rule. Notably, use of bedside ultrasonography to detect pediatric skull fractures is a growing imaging modality for children at risk of skull fracture. Therefore, incorporation of ultrasonography into a minor head trauma decision rule is promising for diagnosis of skull fractures and warrants further investigation.
Our study was limited by its small sample size, and the low frequency of ciTBI led to a large confidence interval, resulting in a lack of power in our results. Our study didn’t collect information on previous medical experience and parental preference, which are clinical factors used by physicians when selecting further investigations in patients at moderate risk for ciTBI. Finally, our study was conducted in a single tertiary care pediatric hospital. Before incorporating the Sainte-Justine Head Trauma Pathway into local practice, it should be validated in a multicentre prospective cohort.
Conclusion
The Sainte-Justine Head Trauma Pathway effectively identifies children younger than two years at risk for ciTBI following head trauma while effectively triaging children at low risk. However, while improving skull fracture detection, the pathway was not a better screening tool than the PECARN rule to identify children at risk for ciTBI.
Footnotes
Partial results of this study were presented at the International Conference on Emergency Medicine (Cape Town, South Africa) in April 2016, the Pediatric Academic Societies conference (Baltimore, USA) in May 2016 and the Canadian Association of Emergency Physicians conference (Québec, Canada) in June 2016.
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception, writing and revision of this article and approved the final version for publication.
- Accepted December 6, 2017.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.