


Abstract
Background: Street and mountain bicycling are popular recreational activities and prevalent modes of transportation with the potential for severe injury. The purpose of this investigation was to compare the incidence, risk factors and injury patterns among adults with severe street versus mountain bicycling injuries.
Methods: We conducted a retrospective cohort study using the Southern Alberta Trauma Database of all adults who were severely injured (injury severity score [ISS] ≥ 12) while street or mountain bicycling between Apr. 1, 1995, and Mar. 31, 2009.
Results: Among 11 772 severely injured patients, 258 (2.2%) were injured (mean ISS 17, hospital stay 6 d, mortality 7%) while street (n = 209) or mountain bicycling (n = 49). Street cyclists were often injured after being struck by a motor vehicle, whereas mountain bikers were frequently injured after faulty jump attempts, bike tricks and falls (cliffs, roadsides, embankments). Mountain cyclists were admitted more often on weekends than weekdays (61.2% v. 45.0%, p = 0.040). Injury patterns were similar for both cohorts (all p > 0.05), with trauma to the head (67.4%), extremities (38.4%), chest (34.1%), face (26.0%) and abdomen (10.1%) being common. Spinal injuries, however, were more frequent among mountain cyclists (65.3% v. 41.1%, p = 0.003). Surgical intervention was required in 33.3% of patients (9.7% open reduction internal fixation, 7.8% spinal fixation, 7.0% craniotomy, 5.8% facial repair and 2.7% laparotomy).
Conclusion: With the exception of spine injuries, severely injured cyclists display similar patterns of injury and comparable outcomes, regardless of style (street v. mountain). Helmets and thoracic protection should be advocated for injury prevention.
Street and mountain bicycling are increasingly popular in North America, with Canadian biking rates exceeding those of the United States.1 In southern Alberta, both bicycling styles are prevalent, given the region’s climate and biking infrastructure.1,2 Chinook winds and reduced snowfall result in improved roadway conditions and warmer temperatures year-round.2 Moreover, about 370 km of bicycling lanes and pathways are available within the city of Calgary, resulting in the largest network of bike paths per 100 000 population in Canada.1,2 Surrounding regions, such as Kananaskis and the Rocky Mountains, further contribute to making the Calgary area one of the busiest biking environments in Canada.
Unfortunately, street and mountain bicycling injuries can be severe and even fatal.3–7 Absolute injury event rates per kilometer for street cycling range from 26 to 68 times higher than those for motor vehicle travel.8 In British Columbia, major trauma related to street cycling occurs at an annual incidence of 49.8 per 100 000 (2.9% of all trauma admissions), with most deaths occurring as a result of neurotrauma.4 Conversely, mountain biking injuries accounted for only 1.6% of all severe trauma patient admissions in this area from 1992 to 2002 (about 1–6 injuries per 100 000 patients per year).5
Although observational studies of bicycling injuries are common,3–7,9–17 to our knowledge, our study is the first to compare the overall major trauma epidemiology of street and mountain bicycling in detail. Few reports have discussed experience with severe bicycling–related multisystem injuries that require emergent surgical intervention or intensive care unit (ICU) admission. Our objective was to compare the incidence, risk factors and injury patterns of street versus mountain bicycling–related major trauma over a 14-year period.
Methods
Using the Southern Alberta Trauma Database, we performed a descriptive retrospective cohort study comparing all adults (≥ 16 yr) who were severely injured (injury severity score [ISS] ≥ 12) while street or mountain bicycling between Apr. 1, 1995, and Mar. 31, 2009. The registry contains prospectively collected data on all trauma patients admitted to the Foothills Medical Centre (FMC), regardless of their length of stay. The FMC is an adult, level 1 tertiary care trauma hospital responsible for all major injuries in southern Alberta, southwestern Saskatchewan and southeastern British Columbia. The University of Calgary Conjoint Health Research Ethics Board approved the study.
The following data were extracted for all severely injured cyclists: demographic characteristics, mechanism of injury, pattern of injury, specific injuries, ISS, mode of transport to hospital, mean patient transport time (i.e., the time from injury to arrival at our trauma centre) and surgical interventions. Although bicycle helmet legislation exists in Alberta and 48.3% of Albertans aged 12 years and older wear a helmet while cycling,18 helmet use is poorly documented in the trauma database as it is often not described in patient charts, emergency medical services (EMS) documents and STARS air ambulance reports. Outcomes included discharge status (alive or dead) and length of hospital and ICU stay. To determine whether there were temporal or seasonal influences on the rate of bicycling-related injury, we also examined the incident date, season and time of day (early morning, 12:01 am–8:00 am; morning/afternoon, 8:01 am–4:00 pm; evening, 4:01 pm–8:00 pm; or night 8:01 pm–12:00 am), as well as whether the injury occurred on a weekend (between 5:00 pm on Friday and 8:00 am on Monday) or on a weekday.
Statistical analysis
We conducted comparative analyses using Stata software, version 8.0 (Stata Corp.). Normally distributed variables are reported as means and standard deviation (SD), and non-normally distributed data are reported as medians with interquartile ranges (IQRs). We compared means using Student t tests and medians using the Mann–Whitney U test. Differences in proportions for categorical data required Fisher exact or χ2 tests. We considered results to be significant at p < 0.05, 2-tailed.
Results
Over the 14-year study period, 11 772 patients required admission to the FMC for management of injuries with an ISS of 12 or greater. Of these, 258 (2.2%) patients were injured (median ISS 17 [IQR 16–25]) during street cycling (n = 209) or mountain biking (n = 49; Table 1). The clinical characteristics of the 2 cohorts were similar, with the exception that mountain bikers were significantly younger than street cyclists (28 v. 43 yr, p < 0.001). Most patients were male (86.4%), and all were operators of the bicycle. Discharge destinations included home (n = 189), rehabilitation facilities (n = 36) and acute care facilities (n = 11). Five patients left against medical advice, and the remaining patients died (n = 17).
Characteristics of the severely injured cyclists included in our study
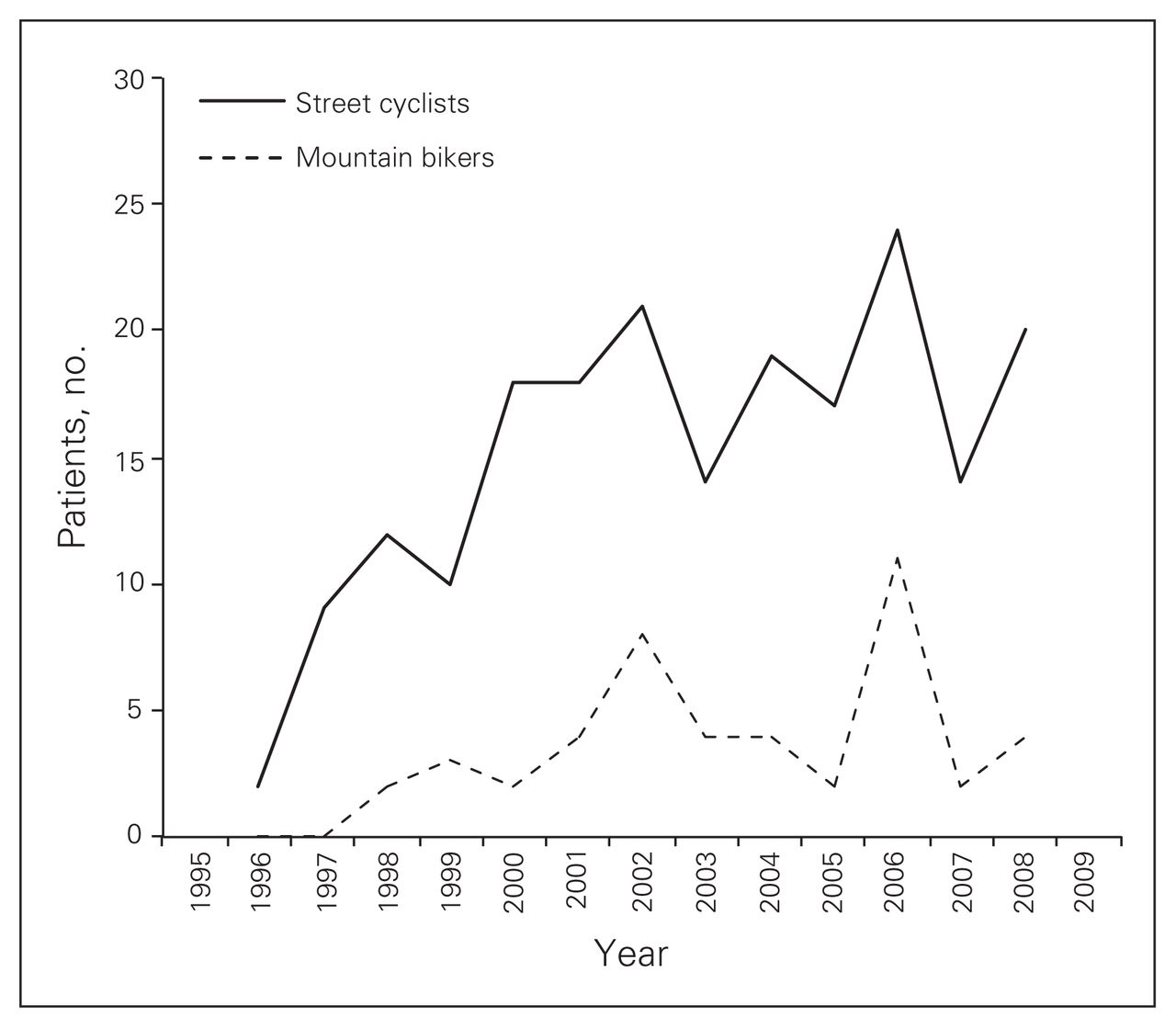
Street cycling was associated with a significantly higher overall rate of admission for severe injury than mountain bicycling (1.8% v. 0.42%, p < 0.001). Although fluctuations occurred across calendar years, there was no significant difference in the yearly rate of admission for either style of bicycling (Fig. 1). The median overall hospital stay for admitted patients was 6 (IQR 3–12) days and was similar between the 2 cohorts. Admission to the ICU was required for 53 (25.4%) street and 15 (30.6%) mountain cyclists (both p > 0.05; similar median ICU stay of 3 [IQR 1–3] d).
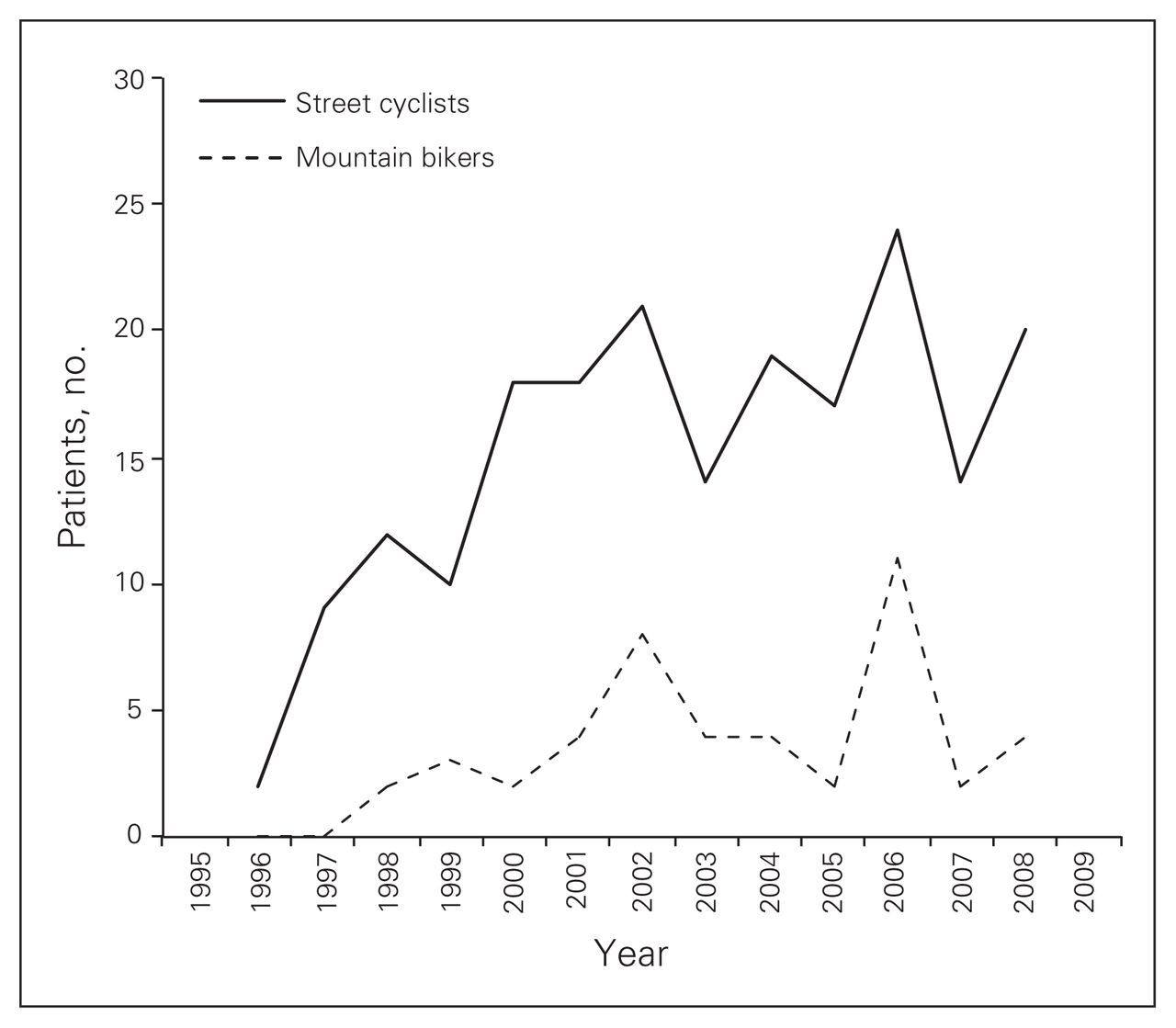
Annual number of trauma centre admissions for severe street and mountain bicycling injuries between 1996 and 2008. The years 1995 and 2009 were excluded, as those calendar years were incomplete in this investigation. No significant difference in annual admission rate was observed between street and mountain bicycling or between any 2 years for either style of bicycling.
The time of day and season during which most bicycling-related trauma occurred was similar for street and mountain cyclists, with most injuries occurring in the morning or afternoon (24.0%) and in summer (53.9%) or spring (29.5%). A trend toward a greater number of bicycling injuries in the summer (53.9%) versus other seasons was observed (p = 0.09; Table 2). When compared with street cyclists, mountain bikers were admitted to hospital more commonly on weekends (61.2% v. 45.0%, p = 0.040).
Individual or environmental characteristics associated with severe bicycling trauma
Most injured cyclists were transported to hospital via ground (74.4%) versus air ambulance (16.7%) or private vehicle (7.9%; Table 1). More mountain than street cyclists were transported by air ambulance (36.7% v. 11.9%, p < 0.001). Conversely, transport by ground was significantly more common for street than mountain cyclists (79.0% v. 55.1%, p < 0.001). Accordingly, the mean transport time was significantly longer for mountain (43 [IQR 22–89] min) than street cyclists (19 [IQR 12–60] min; p = 0.020).
Cyclists’ mechanisms of injury are presented in Table 3. Major injury among street cyclists occurred commonly after being hit by a motor vehicle (27.8%), whereas mountain bikers were often severely injured after faulty jump attempts or bike tricks (20.4%) and falls off cliffs, roadsides and embankments (16.3%; all p < 0.05).
Specific mechanism of injury distribution*
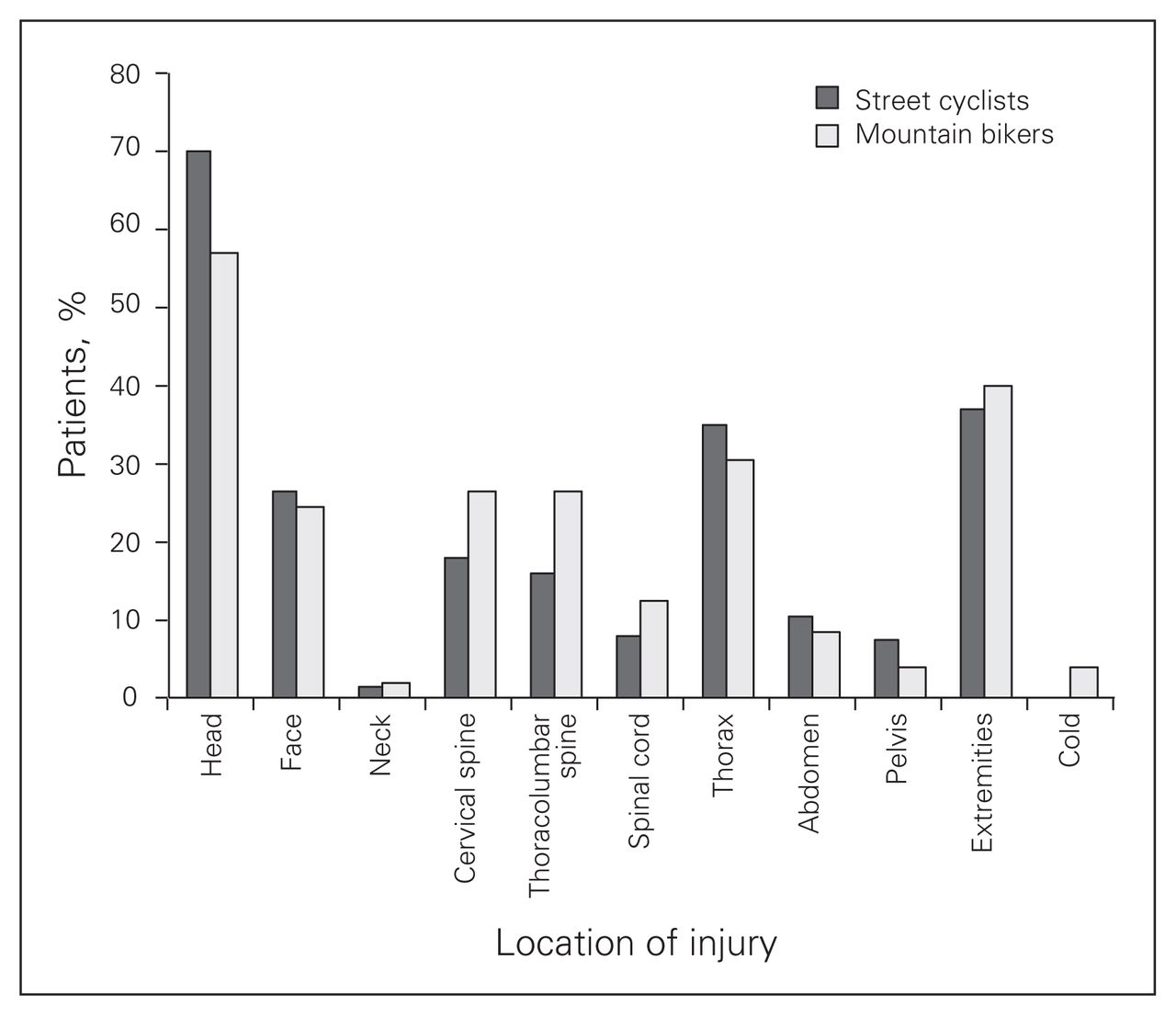
These injury mechanisms resulted in largely similar anatomic injury patterns across both groups (all p > 0.05), with trauma to the head (67.4%), extremities (38.4%), chest (34.1%), face (26.0%) and abdomen (10.1%) being common. Spinal injuries, however, were significantly more frequent among mountain cyclists (65.3% v. 41.1%, p = 0.003; Fig. 2). Specific injuries are described in detail in Table 4.
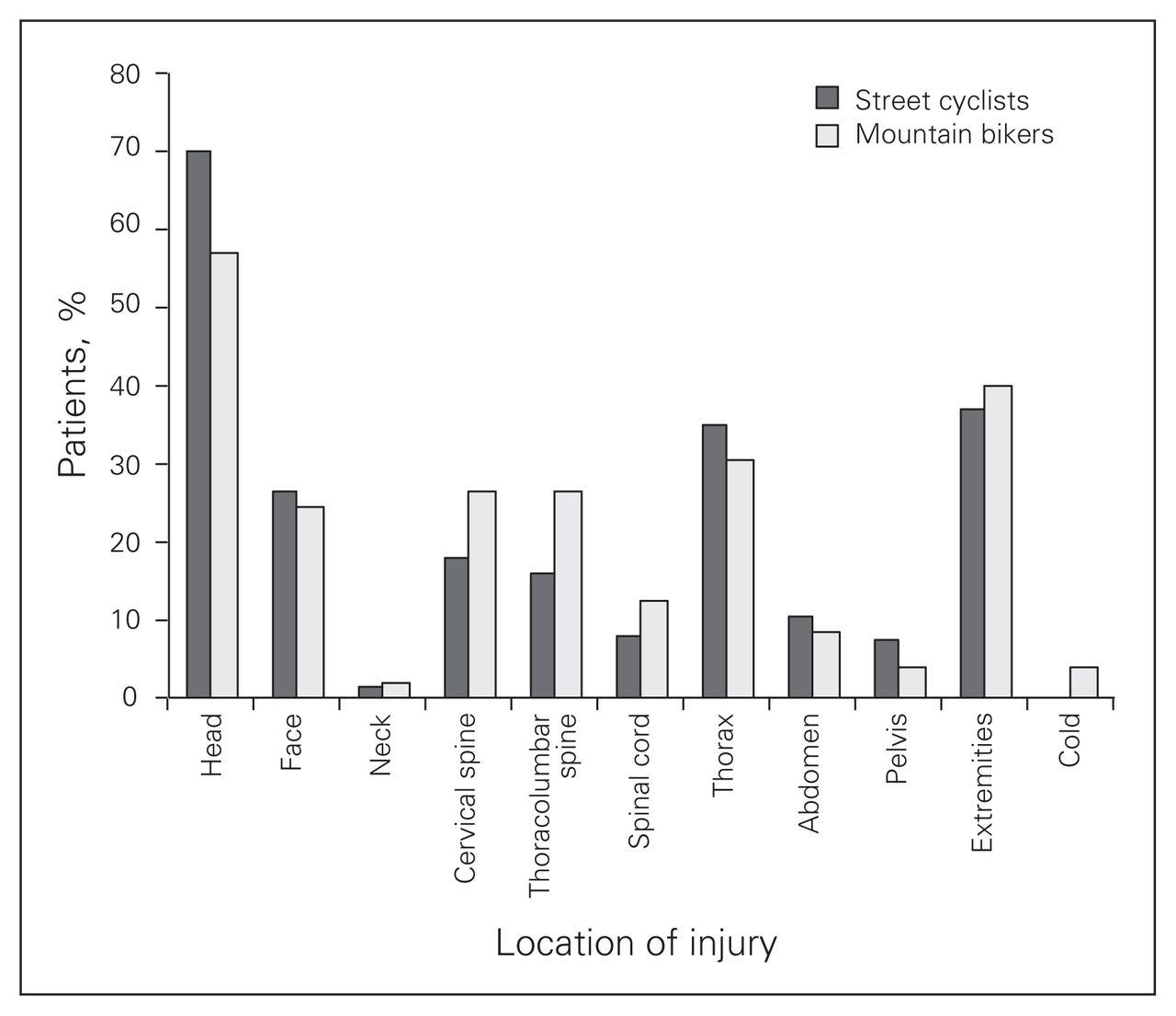
Anatomic injury distribution for the 258 severely injured street and mountain cyclists. Injury rates were all similar between both groups (all p > 0.05).
Specific bicycling-related injuries*
Surgical intervention was required in 33.3% of patients and was similar between groups (Table 5). Extremity open reduction internal fixation was most common (9.7%), followed by spinal fixation (7.8%), craniotomy (7.0%), facial fracture repair (5.8%) and laparotomy (2.7%). Indications for laparotomy included renal laceration (n = 1: American Association for the Surgery of Trauma [AAST] grade III), splenic injuries (n = 4: 3 AAST grade V, 1 grade III), duodenal laceration (n = 1: AAST grade III) and pelvic fracture (n = 1) requiring extraperitoneal packing after pelvic angioembolization.
Surgical interventions performed and associated indications*
A total of 240 (93.0%) patients were discharged alive. Of the 17 (6.6%) cyclists (16 street cyclists and 1 mountain biker) who died from their injuries, 14 had a severe traumatic brain injury (3 also had an extensive extra- or intracranial cerebrovascular artery dissection and another had an associated complete atlantoaxial dislocation), 1 sustained a complete spinal cord injury at the C1/C2 level and 2 succumbed to a combined blunt thoracic aortic injury, open book pelvic fracture and internal iliac artery laceration or an AAST grade II liver and grade III renal injury.
Discussion
Although several investigations have delineated the injury epidemiology of less severely injured cyclists,9,10,12–17,19 this retrospective cohort study analyzed only patients with severe multisystem injuries (ISS ≥ 12). This was affirmed by an overall median ISS of 17, ICU admission rate of 26.4%, surgical intervention rate of 33.3% and mortality of 6.6%. The associated anatomic injury patterns and trauma epidemiology of these patients appear to differ markedly from those of less severely injured cyclists.
In addition to variances in injury mechanisms between street and mountain cyclists, we identified several risk factors for severe cycling-related trauma. Overall, injury was more frequent among street cyclists, possibly because street cycling is an extremely prevalent, year-round mode of transportation in southern Alberta. This finding could also have resulted from some mountain bikers receiving care at hospitals in surrounding mountain regions rather than at the FMC. However, we believe this to be an unlikely explanation, as the FMC is the receiving hospital for major trauma for southern Alberta, southwestern Saskatchewan and southeastern British Columbia. Although bicycle-level falls were the most common injury mechanism, street cyclists were commonly injured after being hit by a motor vehicle, whereas mountain bikers were often injured after faulty jump attempts, bike tricks and falls off cliffs, roadsides and embankments. As expected, most injuries occurred in the morning or afternoon and in summer or spring. Compared with street cyclists, mountain bikers were also more commonly admitted on weekends, likely because a commute to the mountains is often desired.
As reported in other studies,3–7 traumatic brain injury was common, occurring in 67% of severely injured street and mountain cyclists. Up to 7% of these patients required an emergent craniotomy. Interestingly, this injury rate is identical to that reported by Guichon and Myles11 in their pioneering 1975 survey of bicycling-related trauma in Cal-gary. In accordance with a National Trauma Databank study, we identified cerebral contusion (22%), subarachnoid hemorrhage (22%) and subdural hematoma (26%) as the most frequent types of brain injury.6 Epidural hematomas were also common among severely injured cyclists (9%). This may be owing to the predominance of young men in our study, who are known to possess weak attachments between the dura and inner table of the skull.6 They are also more likely to participate in an aggressive, high-speed riding technique.6 Although helmet use reduces the odds of head injury by 63%–88%,20 the frequency and effectiveness of this intervention could not be determined in our cohort, as helmet usage was poorly documented.
Spinal injury was also common (45.7%) and resulted in concomitant injury to the spinal cord in 8.5% of patients. The rate of spinal trauma was significantly higher among mountain than street cyclists (65.3% v. 41.1%, p = 0.003), with fractures to the cervical and thoracolumbar spine being equally frequent.5 A potential mechanism for concomitant head and cervical spine injury in mountain bikers has previously been postulated to involve a fall over the handlebars, resulting in a blow to the top of the head and cervical flexion or hyperextension.5,21 This mechanism may easily have occurred in this study, given that so many mountain bikers were observed to fall off cliffs, roadsides and embankments.
In addition to head and spinal trauma, many street and mountain cyclists also presented with extremity (38%), thoracic (34%) and abdominal injuries (10%). Although the orthopedic injury rate approximated those observed in previous investigations,4–6,22,23 the frequency of thoracic injuries was significantly higher. This most commonly comprised rib fractures, pulmonary contusions and hemo-pneumothoraces. Similar to the rate of chest trauma among horseback riders in our area,24 chest trauma may be underappreciated in severely injured cyclists, highlighting the potential importance of thoracic protection. While reports of subcapsular and central liver hematomas were common before the elimination of upright bicycle handlebars,14,25 the liver was uncommonly injured (1.9%) compared with the spleen (5.4%) among our cohorts.
A total of 17 patients died over the 14-year study period. These deaths were primarily a result of traumatic brain injury, cervical spinal cord injury and/or physiologic exhaustion from ongoing hemorrhage. This is supported by Fife and colleagues,22 who observed that the causes of bicycling-related deaths included early (hemorrhage, cerebral edema and aspiration) and late (pneumonia and pulmonary embolism) etiologies. Age, ISS and alcohol consumption have also been found previously to be associated with increased mortality among injured cyclists.3,6,22
Limitations
Although, to our knowledge, this study is the only comparison of major injuries between street and mountain cyclists, it has several limitations. Given the retrospective design, the possibility of bias cannot be eliminated. Moreover, the most glaring omission was poor documentation of helmet usage, which was unavailable for 85% of all patients identified in the trauma database. Although 48.3% of Albertans older than 12 years wear a helmet while cycling,18 helmet use is frequently not described in patient charts, EMS documents and STARS air ambulance reports. All other variables were well described. Finally, we were unable to characterize individual cyclist skill level, which may impact both injury rates and severity.
Conclusion
The overall rate of trauma centre admission for severe bicycling-related injuries in southern Alberta over 14 years was 2.2%. This was composed primarily of street cyclists. Despite differing style (street v. mountain), severely injured cyclists display largely similar injury patterns with comparable outcomes. While more mountain bikers are injured on weekends, they require surgical interventions at the same rate as street cyclists. Helmet and thoracic protection should be advocated as injury prevention measures.
Acknowledgment
We thank Mrs. Corina Tiruta for assistance with statistical analyses.
Footnotes
This study was presented at the 2011 Canadian Surgery Forum in London, Ont. on Sept. 16, 2011.
Competing interests: None declared.
Contributors: D.J. Roberts, J.-F. Ouellet, F.R. Sutherland and C.G. Ball designed the study. D.J. Roberts, F.R. Sutherland, R.N. Lall and C.G. Ball acquired the data. D.J. Roberts, J.-F. Ouellet, F.R. Sutherland, A.W. Kirkpatrick and C.G. Ball analyzed the data. D.J. Roberts and C.G. Ball wrote the article. All authors reviewed the article and approved its publication.
- Accepted May 22, 2012.
References
In this issue

{kind=link}
{kind=link}
Article tools





