


Abstract
Background: Early and intermediate results have shown that the SB CHARITÉ III total disc arthroplasty (TDA) favourably compares to spinal fusion, but is associated with fewer complications and higher levels of satisfaction. We sought to prospectively report the clinical and radiographic results of the CHARITÉ III TDA after an average of 55 months follow-up.
Methods: We conducted a prospective study of patients receiving the CHARITÉ TDA at either L4–5 or L5–S1 between April 2001 and November 2006. The primary indication for surgery was discogenic low-back pain confirmed by provocative discography. Assessment included pre- and postoperative (3, 6 and 12 mo and yearly thereafter) validated patient outcome measures and radiographic review.
Results: Fifty-seven of the potential 64 (89%) patients were available for complete follow-up. Their mean age was 39 (range 21–59) years. A statistically significant improvement was demonstrated between all the mean pre- and postoperative intervals for the Oswestry Disability Index, visual analogue scale for back and leg pain, and Short Form-36 health survey (p < 0.001). The mean sagittal rotation was 6.5° (range 0.5°–22.4°), and the mean intervertebral translation was 1.1 mm (range 0–2.4 mm). Subsidence of the implant was present in 44 of 53 (83%) patients with an L5–S1 disc arthroplasty. The mean subsidence was 1.7 mm (range 0–4.8 mm).
Conclusion: The 2- to 7-year follow-up of this cohort of patients demonstrated satisfactory clinical and radiographic results in a carefully selected patient population. The radiographic assessment confirmed preservation and maintenance of motion at the replaced disc during the period of follow-up.
Lumbar spine fusion remains a treatment option for the management of patients with low-back pain due to degenerative disc disease for whom nonoperative options have failed. However, spinal fusion has been related to the development of facet joint arthrosis, degeneration of the discs adjacent to the fusion, spinal stenosis, instability and dysfunction of the sacroiliac joints.7–11 In a study of 215 patients who underwent lumbar fusion, a reoperation rate of 27% was reported at a mean follow-up of 6.7 years for adjacent level disease.8 Similarly, in another study, adjacent level disease resulted in a 20% reoperation rate after 2–15 years of follow-up.9
To prevent possible consequences of lumbar fusion, the total disc arthroplasty (TDA) was introduced as an alternative to fusion. It is theorized that an artificial disc replacement preserves motion at the operated levels and reduces the strain on adjacent levels, thus minimizing the chance for development of adjacent level disease. This theory has been supported in biomechanical cadaveric studies; the CHARITÉ TDA was shown to restore motion to the level of the intact segment in flexion–extension, lateral flexion and axial rotation, reproducing a motion very similar to the physiologic motion of an intervertebral disc.13,14 A number of clinical studies also demonstrated preservation of motion at the operated level.15,16
Early and intermediate results have shown that the SB CHARITÉ III TDA (DePuy Spine) favourably compares with spinal fusion and is associated with fewer complications and higher levels of satisfaction than fusion.16–22 Limited long-term clinical results have confirmed the safety and efficacy of this artificial disc.16,20 Most studies have been performed outside of North America, except for those associated with the ongoing United States Food and Drug Administration randomized prospective multicentre clinical trial of the CHARITÉ disc replacement versus lumbar fusion.20 To our knowledge, ours is the first Canadian study that reports the results of lumbar TDA.
The purpose of our study is to prospectively report the clinical and radiographic results of the SB CHARITÉ III TDA performed at our Canadian centre with a minimum of 2 years of follow-up.
Methods
Between April 2001 and November 2006, we prospectively followed 64 patients after they received a CHARITÉ artificial TDA. The primary indication for surgery was discogenic low-back pain. Inclusion and exclusion criteria were similar to those reported by previous studies.20,25 Inclusion criteria were a single-level symptomatic degenerative disc disease (DDD) on magnetic resonance imaging (MRI) that was confirmed by provocative positive discography and associated with persistent symptoms of primarily back and, in some cases, leg pain without overt nerve root compression, an Oswestry Disability Index (ODI) score of 30 or more, a visual analogue scale (VAS) score of 40 or more and failure to respond to a minimum of 6 months of nonoperative treatment. In addition, the patient had to be able to tolerate an anterior abdominal approach.
Exclusion criteria were more than 3 mm of spondylolisthesis or retrolisthesis, osteoporosis, spinal deformity greater than 11°, 2 or more levels of DDD, facet joint arthrosis, previous thoracic or lumbar spine fusion and the presence of current or previous lower lumbar fractures.
All patients included in this study were informed of the option of disc arthroplasty or fusion. The risk and benefits of each procedure were thoroughly discussed, and they consented to be followed prospectively for the purpose of this study. Our hospital ethics review board approved the study protocol.
Operative technique
The surgical approach used was the transperitoneal approach, performed by a vascular surgeon. The surgical technique has been well described previously.26 Particular attention was given to preparation of the end plates. Care was taken to achieve flat end-plate surfaces extending to the posterior aspect of the vertebral body to maximize bone metal contact area. A curette or burr was used to remove any posterior ridge or osteophytes that might limit appropriate posterior posturing of the prosthesis end plate during final insertion.
The patients were mobilized as tolerated on the first postoperative day and instructed to avoid lumbar extension beyond neutral for a period of 6 weeks postoperatively.
Outcome assessment
Outcome evaluation took place preoperatively and postoperatively at 3, 6 and 12 months and once a year thereafter. Validated subjective outcome measures included the ODI, VAS and Short Form-36 (SF-36) health survey version 2. We calculated the VAS separately for leg and low-back pain, assessing both pain frequency and pain intensity. We determined the SF-36 mental component summary score (MCS) and physical component summary score (PCS).
Preoperatively, we obtained an MRI scan and a discogram of the symptomatic degenerate disc to identify surgical candidates. Pre- and postoperative radiological assessment included standing anterior–posterior (AP) and lateral lumbar radiographs in the neutral position, extension and flexion. We used lateral radiographs to assess angle of sagittal rotation (AOR), intervertebral translation of the cephalad on the caudal vertebra, anterior vertical motion (AVM) of the prosthesis and posterior vertical motion (PVM) of the prosthesis. The AOR measured total motion between flexion and extension radiographs by determining the angle subtended between perpendiculars to the superior and inferior end plates of the replaced disc space. The AVM represented the difference between flexion and extension in the vertical distance between the anterior edge of the superior and inferior prosthetic end plates. We calculated the PVM in a similar manner using the posterior edges of the superior and inferior prosthetic end plates to determine the difference in distance between flexion and extension. We used the Cobb technique to determine the lumbar lordosis using the superior end plate of both L1 and S1. We used a T2 midsagittal MRI scan to measure the preoperative anterior and posterior disc heights. We measured the postoperative anterior and posterior disc height using digitized radiographs of the lumbar spine in the neutral position.
We compared postoperative radiographs with preoperative radiographs to detect evidence of adjacent level degeneration above and below the TDA, based on disc space height loss, sclerosis and osteophyte formation.
In addition to the above measurements, we noted the subsidence of the metal component of the artificial disc. Subsidence describes the depth of migration of the metal component of the artificial disc into the vertebra body, and this depth was measured as the distance between the posterior part of the metal component of the prosthetic disc that migrated into the vertebra body and the surface of the end plate of the vertebra (Fig. 1).
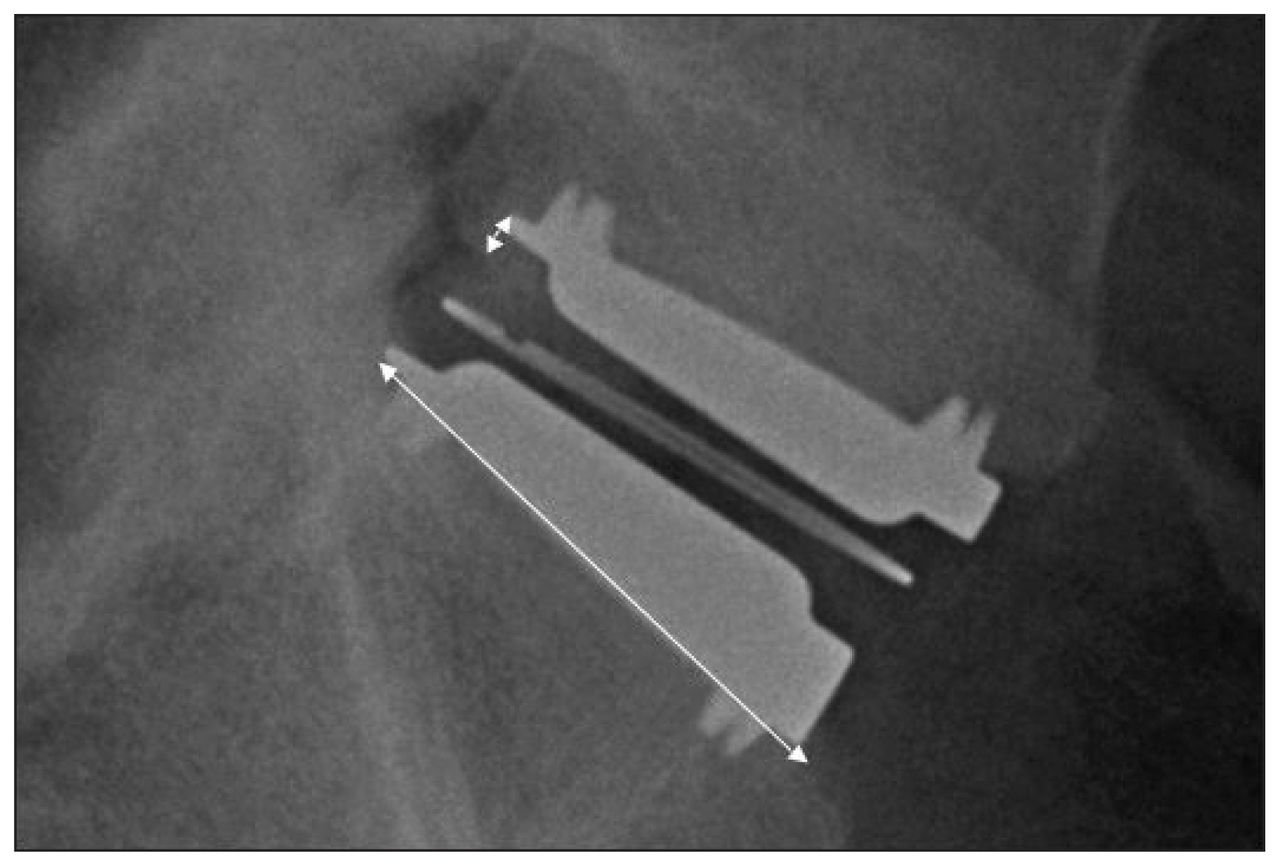
Measurements of subsidence and radiographic disc size.
All measurements were performed using Centricity Picture Archiving & Communications System, version 1.0 (GE Medical Systems). The ratio of magnification was calculated by dividing the actual anterior–posterior artificial disc dimension with the radiographic dimension measured on a lateral radiograph. This magnification ratio was then used to correct the magnification error in all the other measurements. Two of us (M.K. and K.I.) obtained the measurements. Intra- and interobserver reliability was assessed using the intraclass correlation (ICC).
Results
Patients
Sixty-four consecutive patients enrolled in this prospective study: 39 women and 25 men. The mean age at time of surgery was 39 (standard deviation [SD] 7.7) years. Seven (11%) patients were lost to follow-up, leaving 57 patients included in our analysis. The mean follow-up was 55 (range 24–84) months. The demographic and clinical characteristics of patients are provided in Table 1. Table 2 describes the number of patients reviewed at each follow-up.
Demographic and clinical characteristics at baseline of patients who received a CHARITÉ III artificial total disc arthroplasty
Number of patients reviewed at each follow-up
The mean duration of symptoms was 69 (range 9–240) months. Preoperatively, 43 of 57 (75%) patients reported isolated low-back pain, whereas the remaining 14 (25%) reported a combination of back pain and leg pain. Fifty-five percent of patients smoked at the time of the procedure. Table 3 illustrates the difference in preoperative outcome measures between the smoking and nonsmoking cohorts. The mean time off of work was 9.9 (SD 23.3) months. Eleven percent claimed workers’ compensation status. Seven patients had a previous discectomy, 6 of these were performed at L5–S1.
Comparison of baseline means for clinical outcomes between smokers and nonsmokers
There were 53 TDAs carried out at the L5–S1 level and 4 at the L4–L5. The mean intraoperative blood loss was 220 (range 50–700) mL. The mean postoperative hospital stay was 4.7 (range 2–8) days.
Clinical outcome measures
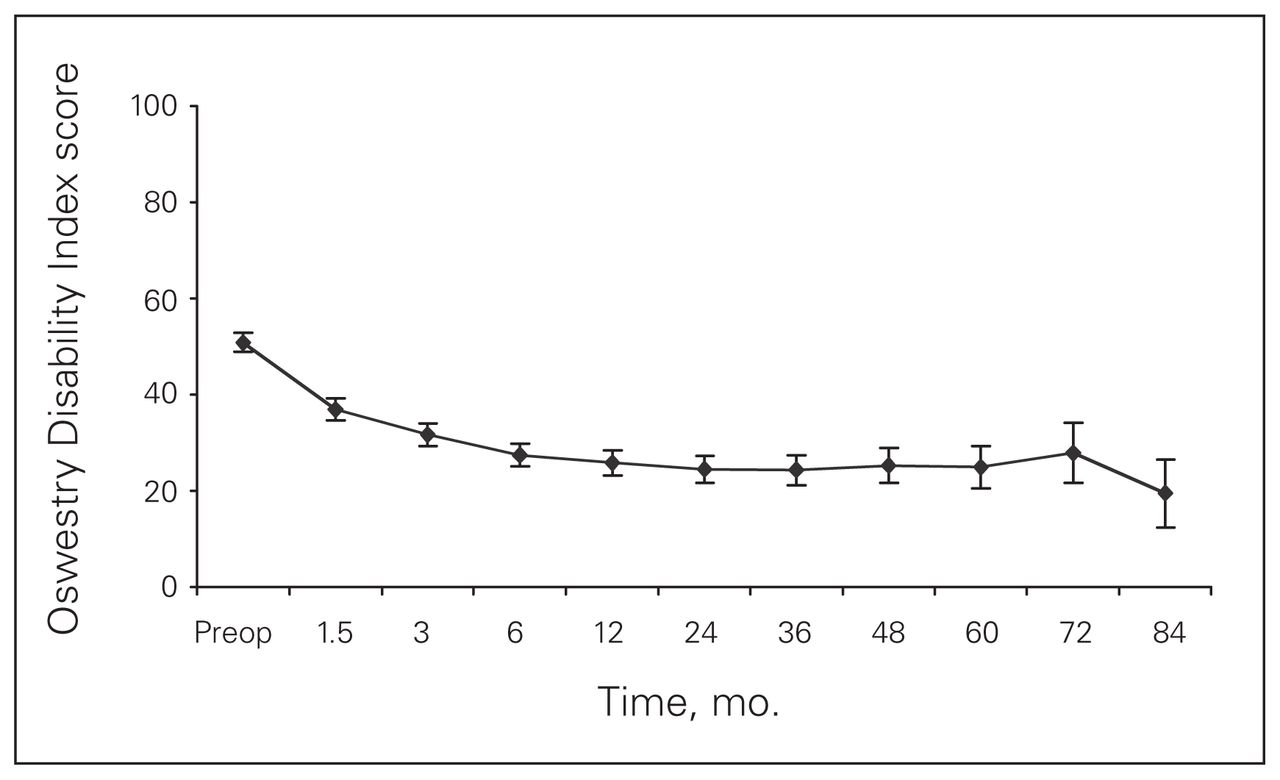
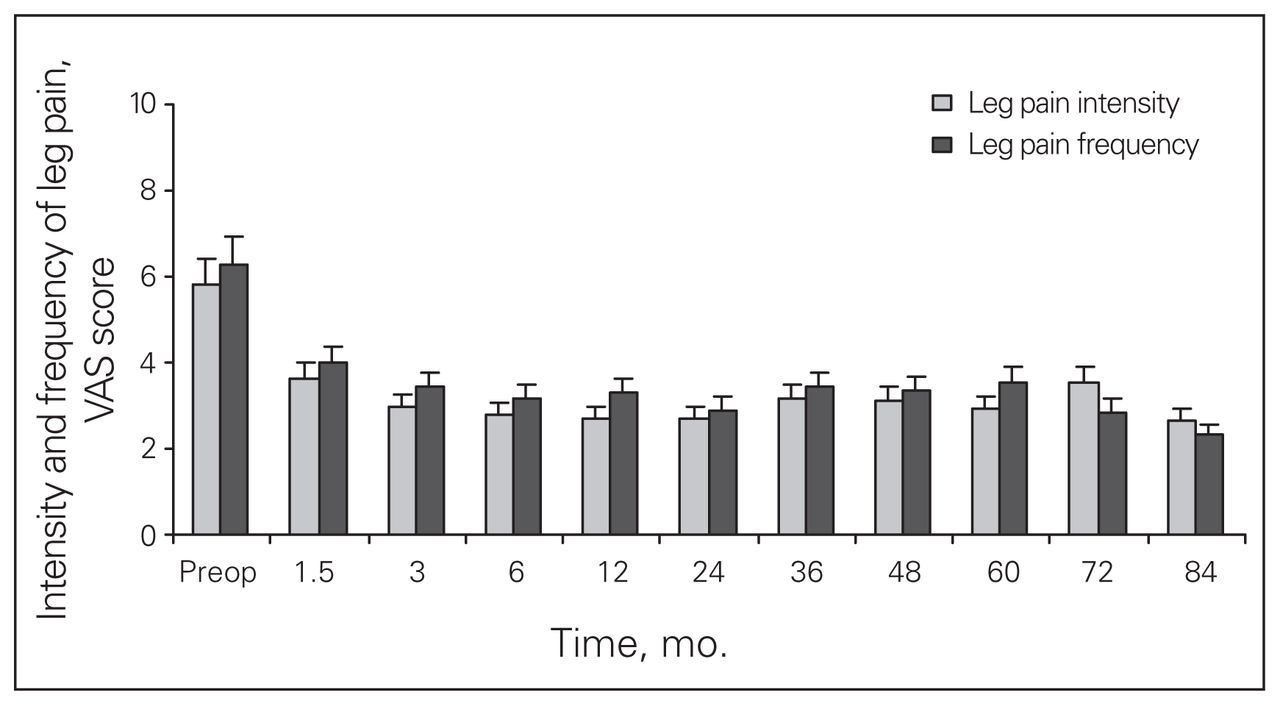
All outcome measures, including the ODI, VAS, MCS and PCS, showed postoperative improvement at the 3-month follow-up (p < 0.001), which persisted during the remaining follow-up period (Figs. 2–5).

Oswestry Disability Index scores of patients who received a CHARITÉ III artificial total disc arthroplasty over 84 months of follow-up.
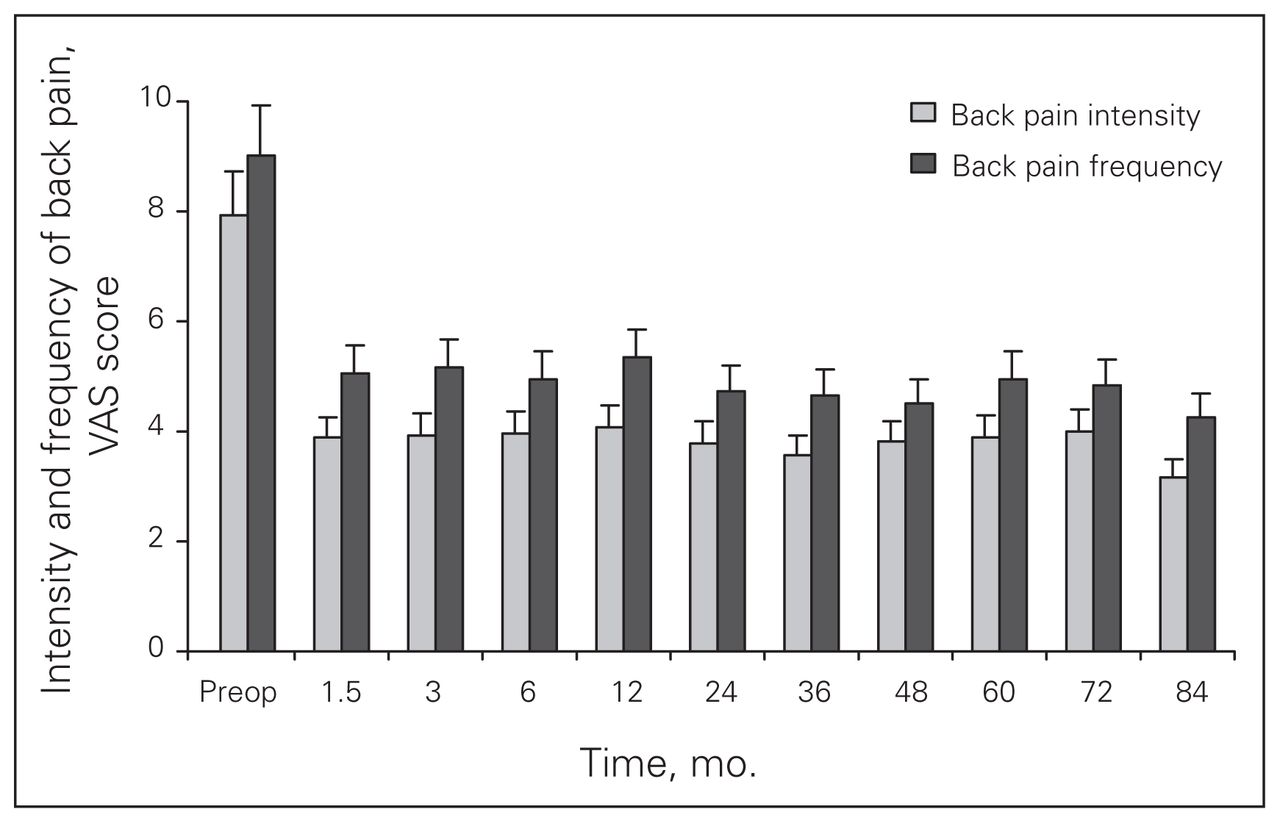
Visual analogue scale (VAS) scores for back pain and intensity among patients who received a CHARITÉ III artificial total disc arthroplasty over 84 months of follow-up.

Visual analogue scale (VAS) scores for leg pain and intensity among patients who received a CHARITÉ III artificial total disc arthroplasty over 84 months of follow-up.

Short Form-36 (SF-36) scores of patients who received a CHARITÉ III artificial total disc arthroplasty over 84 months of follow-up.
Complications
There were 3 (4.7%) early complications: 1 patient experienced a superficial abdominal hematoma, which was treated conservatively, 1 experienced a retroperitoneal hematoma that required exploration and evacuation and 1 of the 27 male patients presented with retrograde ejaculation. Two patients required revision surgery, representing a late complication rate of 3.1%. The first was a young competitive field hockey player who underwent an L5–S1 disc replacement. This patient, against medical advice, returned to playing field hockey only a few weeks postoperatively and sustained an L5 inferior end plate fracture following a fall. Conservative treatment failed to control her symptoms, and she required a posterolateral instrumented fusion leaving the TDA in situ (Fig. 6). The second patient who underwent an L4–L5 disc arthroplasty was among the very first patients selected for disc replacement. In retrospect, preoperative MRI scans demonstrated that this patient had some evidence of adjacent level degeneration at the L5–S1 level and despite a technically adequate procedure at the L4–L5 level continued to have low-back pain. A L5–S1 posterolateral instrumented fusion was performed by another surgeon and therefore it is not possible to comment on the severity of her symptoms before the fusion procedure or on the exact location of the painful segment (replaced L4–5 or L5–S1). In total, the reoperation rate was 4.7% (3 patients).

L4–L5 fusion following an interior end plate fracture resulting in acute subsidence of total disc arthroplasty and severe low-back pain.
Radiographic outcome
Table 4 reports the results of the motion assessment performed at the last follow-up. There was a statistically significant increase (p < 0.001) in the postoperative compared with preoperative lumbar lordosis (Fig. 7). The mean anterior disc height and posterior disc height increased by 2.4 times the preoperative height (Table 5). Subsidence was present in 44 of 53 (83%) patients at the L5–S1 level and was exclusively seen at the posterior part of the inferior end plate of L5. The mean subsidence was 1.7 (range 0–4.8) mm, measured at 3 months after surgery. Although there was a marginal progression of subsidence beyond this time point, it was not statistically significant. Subsidence had no effect on the range of motion at the replaced segment and did not correlate with clinical outcome. In patients who underwent an L4–5 TDA, subsidence occurred at both end plates: mean subsidence was 0.9 mm at the inferior end plate of L4 and 1.75 mm at the superior end plate of L5. Comparison between preoperative and postoperative radiographs demonstrated no evidence of adjacent level disease. Reliability of the measurements was very high for both the intra- and interclass correlation (ICC > 0.8).

Mean preoperative and postoperative lumbar lordosis.
Results of the radiographic measurements of motion at the replaced segment
Mean pre- and postoperative disc height
Discussion
The clinical results demonstrate a satisfactory outcome in patients who underwent a TDA in our unit. Our results are similar to those previously published.16–22 As this was a prospective cohort study, no control group was available for comparison, so the similarity of the results to other published cohorts is important to recognize. The results of this cohort fulfill previously described criteria defining success after TDA or fusion, which included improvement in ODI of more than 25% at 24 months postoperatively, no device failure, no major complications and no neurologic deterioration.20 The clinical outcome measures of the current study demonstrate a significant improvement of the ODI of about 50% postoperatively and a similar degree of improvement in the VAS and SF-36. In our series, there were no cases of device failure, no neurologic deterioration and no major complications. This significant improvement in the clinical outcome measures may not just be related to replacement of the degenerative painful disc, but also to unloading of the facet joints following restoration of the disc height and improvement of the lordosis. This theory has been supported by a prospective morphological study of facet joint integrity following a CHARITÉ disc replacement concluding that decreases in subchondral bone density of the facet joint at the replaced segment suggest a reduction in the loading of the posterior column following a disc replacement.27 Furthermore, improvement in the disc height resulted in an increase in the foramen height, which can result in the relief of preoperative leg symptoms produced by degenerative foraminal stenosis.
The complication rate associated with TDA has been reported to be in the range of 1%–40%.25,18,28,29 The results of the current study demonstrate a relatively low complication rate of 4.7% for early and 3.1% for late complications, resulting in a reoperation rate of 4.7%. In a retrospective study of the CHARITÉ TDA, after a minimum 10 years the overall reoperation rate was 10.4%.16 The authors’ view was that both the design and instrumentation changes as well as specific training for TDA procedures resulted in much shorter learning curves and ultimately fewer complications related to technical aspects of the procedure, particularly for surgeons already familiar with the anterior approach to the low lumbar spine.16 One of the 2 revision surgeries in our cohort was performed for persistent low-back pain, likely derived from an adjacent level to the arthroplasty. This reinforces the critical importance of patient selection.
The range in reported complications may be explained by differing surgical approach and technique. Following an anterior approach, 1 patient in our cohort experienced retrograde ejaculation; this compares favourably to a 10-fold increase in the rate of retrograde ejaculation reported using a transperitoneal approach.31 High rates of heterotopic ossification and spontaneous fusion have now been attributed to the surgical technique used at the time of implantation and particularly to the repair of the anterior longitudinal ligament (ALL) following the disc implantation.33 Rates of complete ossification and spontaneous fusion have ranged between 2.8% and 60%.19,32 In our cohort of patients, the ALL was not repaired, and there were no observed cases of heterotopic ossification.
Motion was maintained at the replaced segment. The mean 6.5° of sagittal rotation during flexion and extension compares favourably to the sagittal rotation reported in the literature,31 where at a 5-year follow-up the mean angle of sagittal rotation was 6.0° for the CHARITÉ group of patients compared with 1.0° for the fusion group. An interesting finding in our study was the variation in rotation for our patient cohort, which ranged between 0.5° and 22.4°. We believe this can be explained by a lack of standardization when performing the flexion and extension radiographs. We frequently noticed a substantial inconsistency in rotation among follow-up periods for particular patients. In these patients, despite the fluctuations in sagittal rotation among follow-up periods, clinical outcome measures remained consistent, supporting the concept that the variation in range was related more to patient effort than symptoms.
The mean intervertebral translation in our study was 1.1 mm, the AVM 1.5 mm and the PVM 1.5 mm, which fall within the physiologic range of translation previously described.14 It remains unknown what motion is required at one spinal segment to protect the adjacent segments from degeneration. It is theorized that the restoration or preservation of motion at the replaced segment can only be beneficial for the adjacent segment, provided that this motion follows a pattern close to the physiologic one. No radiographic evidence of adjacent level disease was seen in our cohort of patients; however, we recognize that our follow-up period was relatively short for this to be fully assessed. Subsidence of the metal prosthesis on the end plate was quite common without influencing the clinical outcome and the motion across the replaced segment.
Conclusion
The 2- to 7-year follow-up of this Canadian cohort of patients demonstrated satisfactory clinical and radiographic results in a carefully selected patient population. The radiographic assessment confirmed preservation and maintenance of motion of the replaced disc with a follow-up averaging 55 months.
Footnotes
This work was presented at the meeting of the British Association of Spine Surgeons, Sheffield, England, Feb. 25–27, 2009, and at the Annual Meeting of the Canadian Orthopaedic Association, Whistler, BC, July 3–6, 2009.
Competing interests: None declared.
Contributors: Drs. S. Bailey and Gurr designed the study. Drs. Katsimihas, Issa, Rosas-Arellano and Gurr acquired the data, which they analyzed with Drs. Fleming and C. Bailey. Drs. Katsimihas, Issa and C. Bailey wrote the article, which Drs. S. Bailey, Fleming, Rosas-Arellano and Gurr reviewed. All authors approved publication of the article.
- Accepted March 31, 2010.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.