


Abstract
The potential use of positron emission tomography (PET) imaging in patients with non–small cell lung cancer (NSCLC) is broadly divided into 5 categories: management of solitary pulmonary nodule, mediastinal lymph node evaluation, detection of metastases, evaluation of response to chemoradiation and detection of recurrence. The purpose of this review is to discuss the current clinical applications of 18F-fluorodeoxyglucose PET in patients with NSCLC and to discuss future applications and developments of this technology.
Despite many advances in the diagnosis, staging and treatment of non–small cell lung cancer (NSCLC), the overall 5-year survival rate of patients with resectable NSCLC is less than 50%.1 This suboptimal survival rate is likely due to many factors, including the aggressiveness of the specific phenotype, locally advanced disease at presentation and inaccurate pretreatment staging. It is plausible that undetected locoregional and distant micrometastatic disease at the time of presentation results in suboptimal or at times inappropriate treatment and, therefore, decreased stage-specific survival. Accurate clinical staging at the time of diagnosis has many important advantages, of which the following 3 have particular importance
it allows for appropriate patient selection for potentially curative surgical and/or nonsurgical therapies,
it identifies patients who would benefit from neoadjuvant therapy, and
it allows for more accurate follow-up assessment and detection of loco-regional recurrences that might still be amenable to salvage treatment.
In the management of NSCLC, 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) is an imaging technology with evolving potential. The advantage of FDG-PET lies in its ability to detect metabolic changes in cancer cells even before the manifestation of the anatomic changes commonly identified by conventional imaging modalities such as computed tomography (CT), ultrasonography, magnetic resonance imaging (MRI) and bone scintigraphy. This advantage may help with more accurate staging than is possible with conventional imaging. It may also identify tumours at an earlier stage, assess their response to neoadjuvant therapy and help with follow-up surveillance. The potential capability of PET in assessing the tumour responsiveness to chemotherapy can be used as a prognostic factor, thereby influencing the direction of further management.
The optimal use of FDG-PET in the management of lung cancer continues to evolve. The overall poor prognosis of lung cancer and lack of optimal treatment for advanced stages of the disease have facilitated rapid integration of this imaging technology in the management of NSCLC. However, its financial burden on health care systems and individual payers has brought its widespread use into question. The purpose of this review is to discuss the current practical applications of FDG-PET in patients with NSCLC, summarizing clinically applicable data. A systematic review of the role FDG-PET in the diagnosis and staging of lung cancer has already been published by one of us (Y.U.).2
Basic principles of FDG-PET
18F-fluorodeoxyglucose is a radiolabelled glucose analogue taken up by metabolically active cells that have increased glycolysis capability. This capability is largely related to upregulation of glucose membrane transporters and increased activity of enzymes involved in the glycolytic pathway.3 Once injected intravenously, FDG diffuses into the extracellular space and subsequently is taken up by cells. In the intracellular space, FDG is phosphorylated to FDG-6-phosphate by hexokinase, the first enzyme of the glycolytic pathway. Since FDG-6-phosphate is not a substrate for the second enzyme, glucose-6-phosphate iso-merase, it is not catabolized further and remains trapped in the cells of uptake.4,5
The trapped FDG decays by positron emission. The collision of a positron with an electron produces energy in the form of 2 511-KeV photons that travel in opposite directions. The PET scan detects these annihilation photons and is able to construct an image based on the concentration and distribution of the radioisotope emitted from various point sources. This creates PET scan images that can be displayed in coronal, sagittal or transverse manners.
Normal physiologic uptake of FDG takes place in various organs such as the brain, heart, kidneys, bladder and, to a lesser extent, the liver, stomach, colon, spleen and bone marrow (Fig. 1). The cellular concentration of FDG is characterized by a semiquantitative measurement called standardized uptake value (SUV). 18F-fluorodeoxyglucose uptake in a nonphysiologic region with an SUV greater than 2.5 is considered to be suspicious for the presence of cancer.

Coronal maximum intensity projection image of a normal positron emission tomography scan showing the physiologic uptake of 18F-fluorodeoxyglucose in the heart, kidneys and bladder.
Non–small cell lung cancer
In dealing with primary NSCLC, pathological diagnosis and clinical staging form the basis for further management and treatment. Pathological diagnosis, which is commonly initiated on discovery of a solitary pulmonary nodule (SPN) or mass, is followed by clinical staging that involves the assessment of mediastinal nodal status and search for distant metastatic disease. The PET scan appears to play a role in assessing an SPN, evaluating mediastinal lymph node involvement and detecting distant metastasis (Fig. 2).
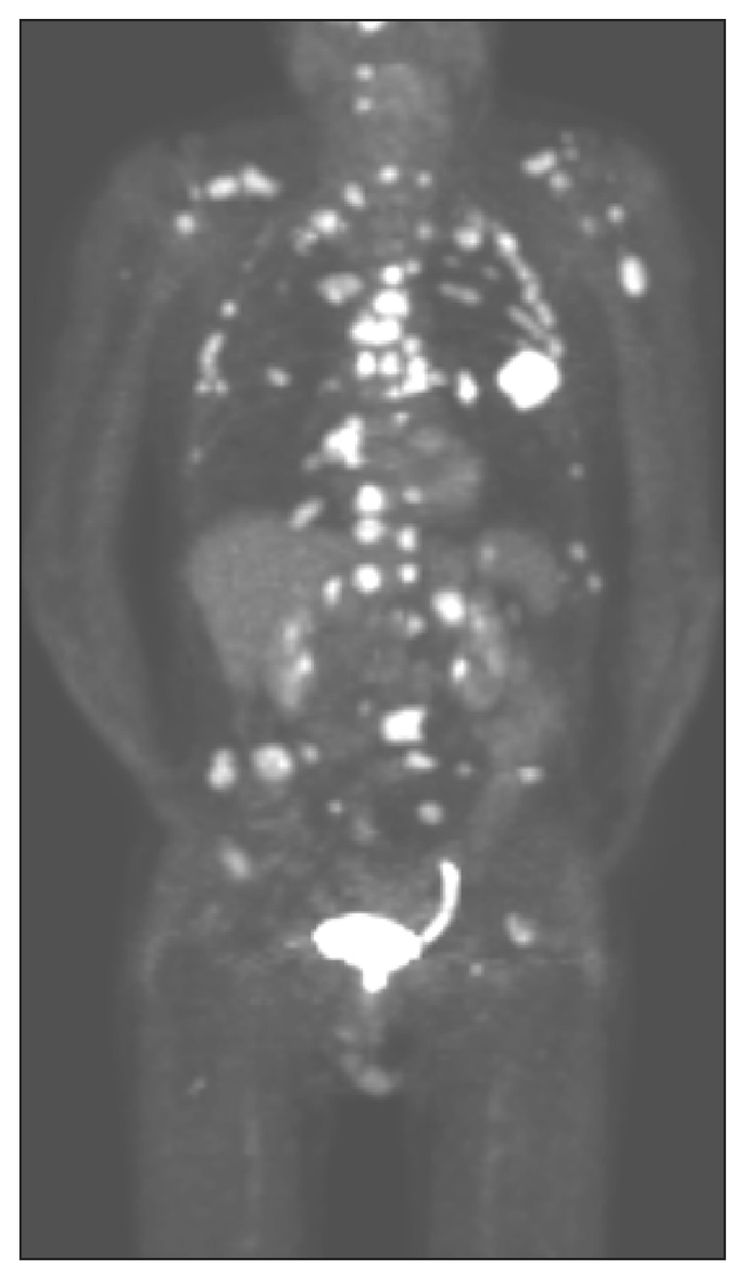
Images of an abnormal positron emission tomography scan showing cancer in the left lung with extensive mediastinal disease and bone metastasis not detected on bone scan, bone radiographs or computed tomography (CT) scans. Only the lung mass was seen on a CT scan. The patient died 1 month later.
Management of an SPN
An SPN, or coin lesion, is defined as a nonspiculated round lesion smaller than 3 cm in diameter without associated atelectasis or adenopathy.6 Larger lesions are likely to be cancerous and prompt pathological diagnosis; subsequent resection is usually indicated. However, 70%–75% of nodules that are labelled as indeterminate based on initial history and standard radiological studies may ultimately be cancerous.7 In view of the primary objectives of managing SPN — namely early detection of lung cancer, avoidance of surgery on benign lesions and efficient use of resources — PET imaging has been shown to help differentiate benign from cancerous lesions as small as 1 cm.8 The sensitivity, specificity and accuracy of PET in differentiating benign from cancerous SPNs are more than 95%, 75% and 90%, respectively.9–12 The false-negative rate of PET for SPN was reported to be less than 5% in one study.13 However, 8 of 20 PET-negative SPNs smaller than 1 cm were proven to be cancerous in another study.14 The cost-effectiveness of adding PET to standard radiological modalities used in the management of SPN is suggested for those larger than 1 cm,15,16 when pretest probability of cancer and CT scan findings is discordant, or in patients with intermediate pretest probability who are at high risk for surgical complications.17 Preliminary analysis of a multicentre cooperative study to determine the accuracy of PET in SPNs larger than 1 cm also suggests higher specificity and the same sensitivity rates as CT scanning.18
Positron emission tomography can be an effective tool in managing SPNs larger than 1 cm, especially if more invasive diagnostic modalities such as transthoracic needle aspiration and bronchoscopy fail to provide tissue for definitive diagnosis. For SPNs smaller than 1 cm, only strong uptake of FDG may be of diagnostic value. Despite the information provided by PET that can influence management, no data exist to support improved overall survival when PET is used in the management of SPNs, as is true with other diagnostic procedures and imaging.
Positron emission tomography has some inherent limitations that should be considered when it is used in the clinical setting. Although FDG has high sensitivity for cancerous conditions, there are benign processes that result in abnormal accumulation of FDG and false-positive images.19–21 These false-positive results are due to conditions where FDG accumulation occurs in metabolically active tissue that is not cancerous. These conditions include infection; chronic or acute granulomatous disease such as sarcoidosis; autoimmune disease such as Grave disease; inflammatory conditions such as postoperative surgical field or radiated field; atherosclerotic plaque; and certain benign tumours such as giant-cell tumour, bony fibrous dysplasia and colonic adenomatous polyps.22–26 False-negative PET images can also occur for low-metabolism tumours such as bronchioloalveolar carcinomas (up to 60%)27 and carcinoid tumours (up to 85%).28,29
The use of PET in diabetic patients may pose a unique challenge because the rate of FDG accumulation in tumours is decreased and tumour targeting with FDG is impaired among these patients; therefore, diabetes may reduce the sensitivity of FDG-PET for lung cancer detection.30 However, it is shown that FDG uptake in lung tumours is not substantially influenced by blood glucose levels in diabetic patients if blood glucose levels are well controlled.31 The accuracy of PET in diabetic patients, as long as the blood glucose levels are under control, is considered to be the same as in the general population.
Positron emission tomography is a valuable tool to evaluate SPNs; however, one must be aware of the causes of false-positive and false-negative results when interpreting SUV. As a recent study suggests, there is a 24% chance that a suspicious nodule with an SUV of 0–2.5 is cancerous.32
Mediastinal lymph node evaluation
Mediastinal lymph node metastasis has a clinically important impact on the course of therapy and prognosis of NSCLC.33 Anatomic lung resection is the standard treatment for resectable NSCLC without evidence of mediastinal and distant metastasis. In the case of ipsilateral lymph node metastasis (N2), neoadjuvant therapy followed by surgery or chemoradiation therapy with curative intent are the accepted treatments.34,35
Traditional mediastinal node assessment is done using a CT scan of the chest and/or mediastinoscopy. A mediastinal node is considered to be abnormal on a CT scan if its shortest axis is greater than 1 cm. In this situation, mediastinoscopy is warranted. The American College of Surgeons Oncology Group Z0050 trial evaluated the addition of PET to routine staging in 303 patients with documented or suspected NSCLC who were found to be surgical candidates.36 Positron emission tomography was significantly better than CT for the detection of N1 and N2/N3 disease (42% v. 13%, p = 0.018 for N1 disease and 58% v. 32%, p = 0.004 for N2/N3 disease), with the negative predictive value close to 90%. This advantage was also supported by a meta-analysis that showed that the median sensitivity and specificity for CT were 61% and 79%, respectively, compared with a sensitivity and specificity of 85% and 90%, respectively, for PET.37 However, the cost-effectiveness of this superiority can only be demonstrated if PET can convincingly replace invasive pathologic evaluation of lymph nodes by transbronchial bronchoscopy, mediastinoscopy or thoracotomy, thereby rendering pathological evaluation of lymph nodes unnecessary (Fig. 3).
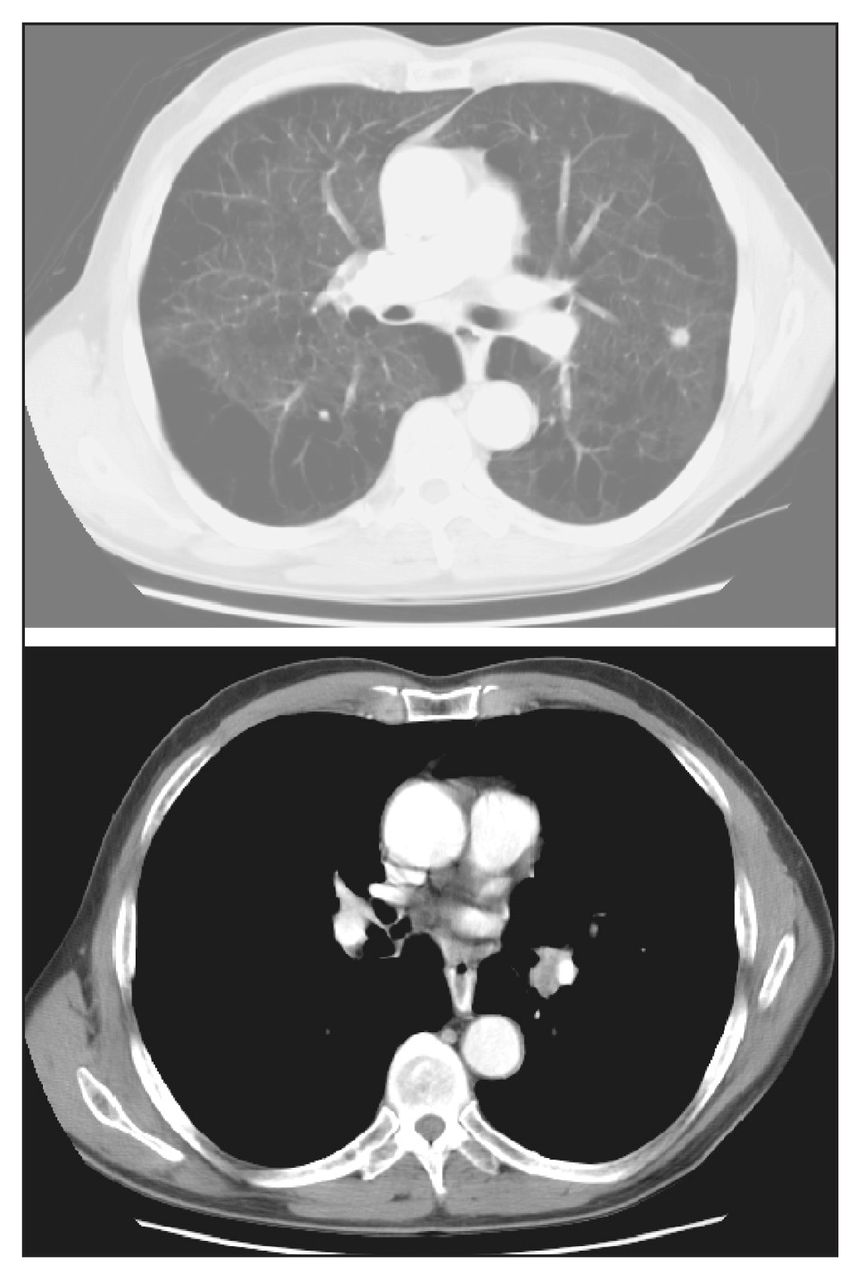
Computed tomography scans of a calcified nodule in the left lung and borderline mediastinal adenopathy in a symptomatic patient. Bronchoscopy and media-stinoscopy were nondiagnostic. A coronal maximal intensity projection positron emission tomography image showing abnormal 18F-fluorodeoxyglucose uptake only in the left hilum. On thoracotomy, hilar nodes were positive for mixed small-and large-cell lung cancer. The left nodule was a necrotizing granuloma.
When compared with mediastinoscopy, the sensitivity, specificity, positive and negative predictive values and accuracy for PET scan for N2/N3 disease were 64.4%, 77.1%, 44.6%, 88.3% and 74.3%, respectively.38 Therefore, a positive PET scan result for mediastinal nodes requires pathological confirmation.39 However, the result of a negative PET scan may negate the requirement of mediastinoscopy for mediastinal nodes that were negative on CT scan.40 This conclusion is supported by a recent meta-analysis reporting a post-test probability for N2 disease of 5% for lymph nodes measuring 10–15 mm on CT scans in patients with negative PET scan results.41
Detection of distant metastases
Metastases from NSCLC occur mostly in the brain, bones, liver and adrenal glands in decreasing order.42 As discussed in the section on PET limitations, this imaging modality has low sensitivity for detecting brain metastases because of the high rate of glucose uptake by brain cells, and therefore it is not recommended for this purpose. Up to 10% of patients with NSCLC have unilateral adrenal mass at presentation,43 of which about 60% are benign.44 Therefore, a number of patients with localized NSCLC and an asymptomatic unilateral adrenal mass require percutaneous biopsy. Positron emission tomography can further decrease the need for biopsy for PET-negative adrenal lesions as its sensitivity and specificity for detecting metastatic adrenal disease are 93%–100%, and 80%–96%, respectively.45,46 The overall accuracy of PET for adrenal lesions identified on CT scans or MRIs is reported to be 92%.47 A PET-positive adrenal lesion, however, should still undergo biopsy to confirm meta-static disease if this is the sole site of metastases.
Bone involvement is usually assessed by 99Tc radionuclide technetium isotope medronate methylene diphosphonate bone scintigraphy, which has a sensitivity, specificity and accuracy of around 90%, 60% and 66%, respectively. Positron emission tomography is reported to have similar sensitivity as bone scintigraphy (90%), but a higher specificity (98%) and accuracy (96%).48 In another study, the accuracy of PET and bone scintigraphy were 94% and 85%, respectively (p < 0.05), sensitivity values were 91% and 75%, respectively, and specificity values were 96% and 95%, respectively.49 Therefore, the findings of bone scintigraphy may, at best, replicate information that can be obtained using PET.
Unsuspected liver metastases occur in 3%–6% of patients with lung cancer who have normal hepatic function.50 The conventional methods for detecting liver metastases are ultrasonography, CT and/or MRI. Although there are no specific series on the use of PET in detecting liver metastases in patients with NSCLC, PET is reported to detect liver metastases in up to 2% of patients who were thought to be free of liver metastases based on conventional imaging.51 Overall, the sensitivity of the liver metastasis detection in patients with other cancers is reported to be higher with PET than other modalities.52 Therefore, by inference, one may conclude that information provided by PET can help characterize indeterminate hepatic lesions suspected of metastases and, in a small number of patients, detect a missed hepatic lesion.
In the American College of Surgeons Oncology Group Z0050 trial,36 6.3% of patients with documented or suspected NSCLC who were found to be surgical candidates based on routine staging procedures had unsuspected metastatic disease or a second primary cancer. Distant metastatic disease found in 6.6% of patients was subsequently shown to be benign. By correctly identifying advanced disease (stages IIIA, IIIB and IV) or benign lesions, it was concluded that the use of PET helped to potentially avoid unnecessary thoracotomy in 20% of patients. This conclusion, however, is challenged by a recent prospective randomized controlled trial involving patients with stage I and II NSCLC.53 In this trial, 92 patients were assigned to the no PET group and 91 were assigned to the PET group. Compared with conventional staging, PET upstaged 22 patients, confirmed staging in 61 and staged 2 patients as benign. Stage IV disease was detected in only 2 patients. This modality led to further investigation or a change in clinical management in 13% of patients and provided information that could have affected management in a further 13% of patients. There was no significant difference between the trial arms in the number of thoracotomies avoided (p = 0.2). Although PET was useful in the clinical management of patients with NSCLC in this group of patients with predominantly stage I disease, its addition did not result in fewer thoracotomies in patients who had careful conventional staging.
Determination of response to chemoradiation
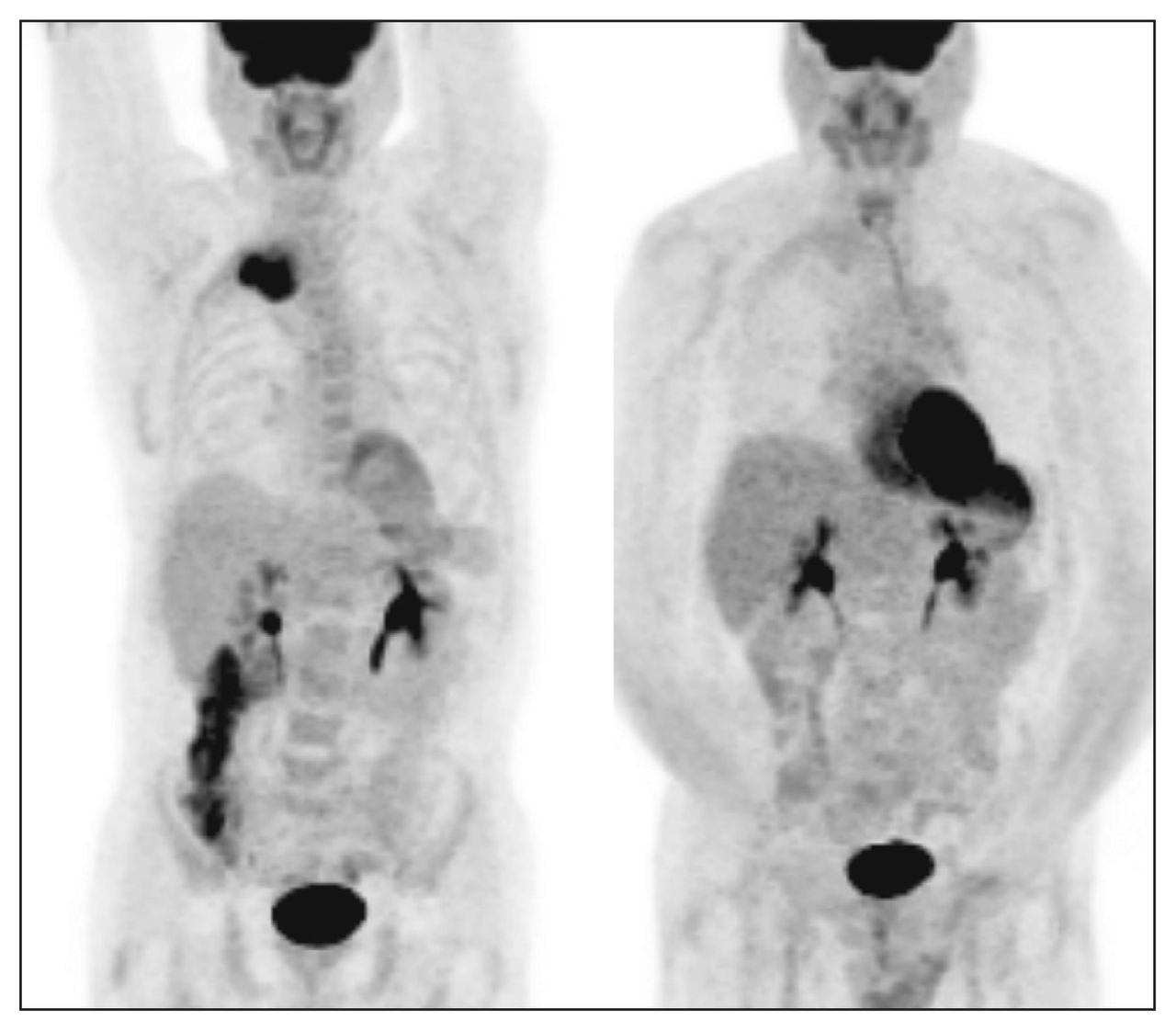
Neoadjuvant chemoradiation therapy followed by curative resection is emerging as an acceptable treatment for resectable NSCLC with pathologically proven nonbulky ipsilateral paratracheal and/or subcarinal mediastinal nodal metastasis (stage IIIa).54 Assessment of response to neoadjuvant therapy may in fact result in the alteration of the course of management and provide prognostic information. This information can also contribute to the management of patients who are offered definitive chemo-radiation (stage IIIb and unresectable stage IIIa) (Fig. 4).
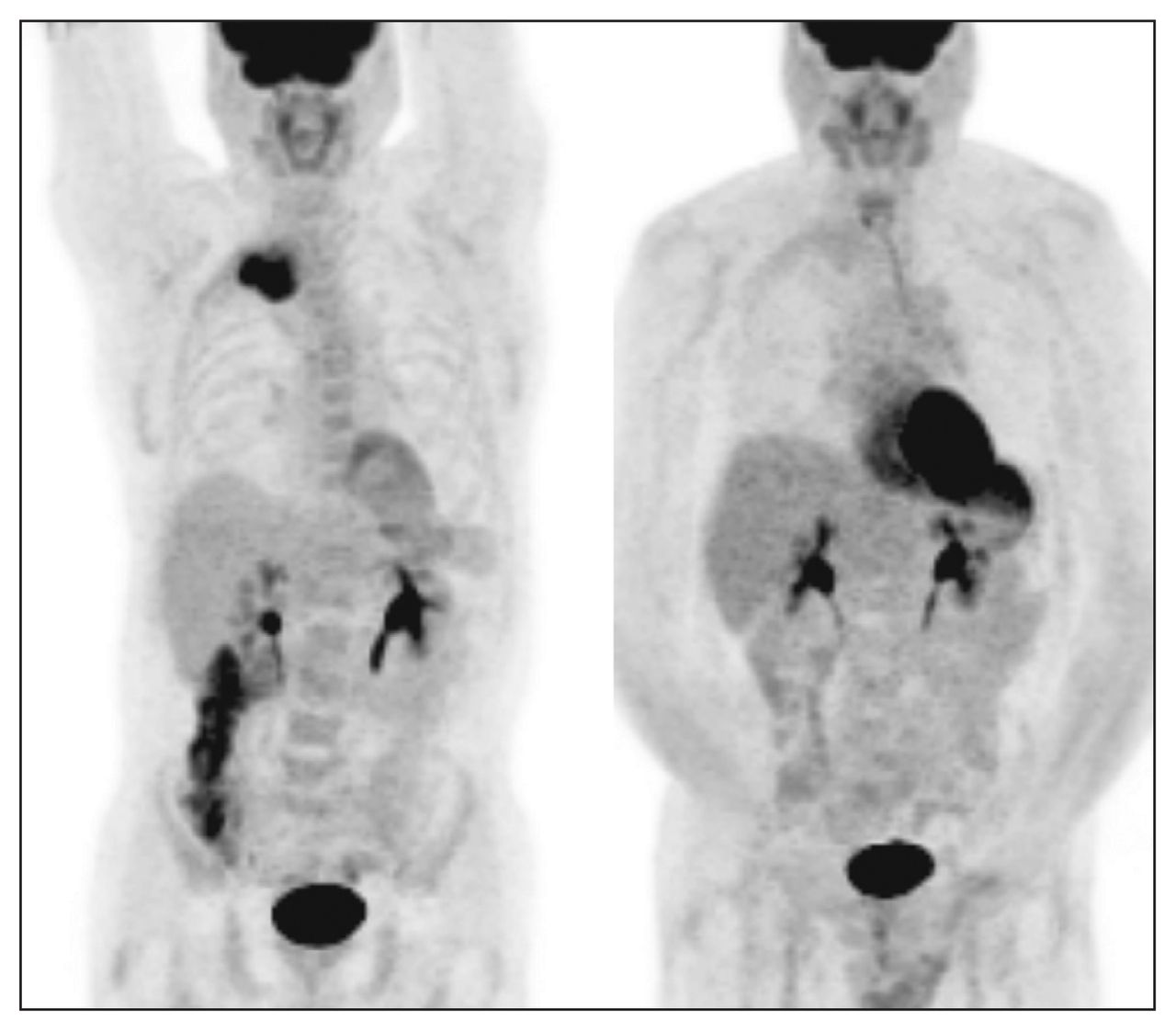
Positron emission tomography scan showing the coronal maximum intensity projection view of locally advanced non–small cell lung cancer (left) before and (right) after completion of neoadjuvant therapy. Decreased 18F-fluorodeoxyglucose uptake suggests tumour response to therapy.
Weber and colleagues55 prospectively evaluated the role of PET in predicting response to chemotherapy in 57 patients with advanced NSCLC who were scheduled to undergo platinum-based chemotherapy. Patients were studied using FDG-PET before and after the first cycle of therapy. A reduction of tumour FDG uptake by more than 20%, as assessed by SUV, was used as a criterion for a metabolic response. The median times to progression and overall survival were significantly longer for metabolic responders than for metabolic nonresponders (163 v. 54 d, p < 0.001 and 252 v. 151 d, p = 0.005, respectively). Cerfolio and colleagues56 also suggested that when the SUV decreased by 80% or more, a complete pathologic response could be predicted with a sensitivity of 90%, specificity of 100% and accuracy of 96%, irrespective of cell type or neoadjuvant treatment.
The Leuven Lung Cancer Group57 examined the value of PET in predicting long-term oncologic outcomes. They analyzed SUV and survival in 91 patients who underwent complete surgical resection. Patients with a resected tumour smaller than 3 cm had an expected 2-year survival of 86% if the SUV was below 7 and 60% if it was greater than 7. Nearly all resected tumours larger than 3 cm had SUVs greater than 7 and an expected 2-year survival of 43%. An SUV of 7 was found to have the best discriminative value for survival. These survival differences are also observed when SUV of primary NSCLC was taken into account in more recent studies.58,59
Detection of recurrence
One of the most important objectives during follow-up after curative treatment of NSCLC is detection of recurrence. Most of the current imaging techniques are sensitive for structural changes but have limited ability to distinguish scars from viable tumours. The sensitivity and specificity of PET for detecting recurrence of primary NSCLC are shown to be 93%–100% and 89%–92%, respectively.60–62 These data suggest that PET is superior to CT, with a sensitivity of 71% and specificity of 95% for detecting recurrence. A recent study has also suggested that SUV in recurrent tumours is an independent prognostic factor in patients with recurrent NSCLC.59
It should be emphasized that the apparent superiority of PET over standard imaging modalities in detecting recurrence is based on retrospective pilot studies with small numbers of patients. Therefore, the clinical significance of this potential superiority is still unknown, as early detection of local recurrence is of value only if there is a salvage therapy available and if there would be potentially no advantage to the early detection of distant recurrence.
Future applications and developments
Role of integrated PET/CT in the management of NSCLC
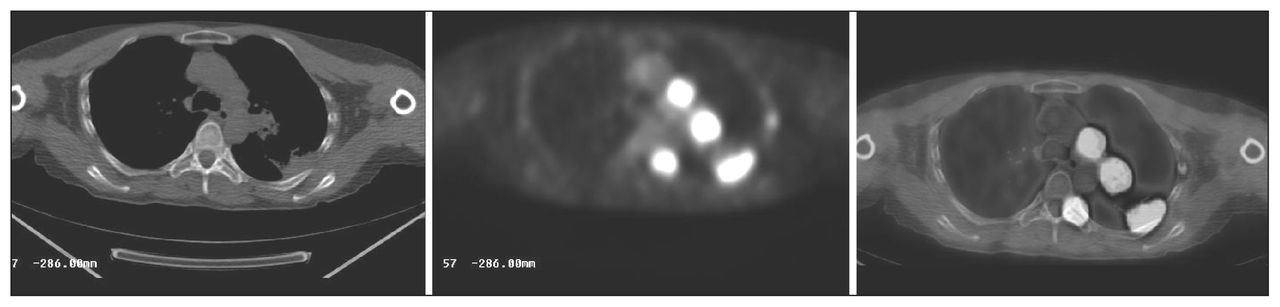
Integrated PET/CT technology has the advantage of combining the metabolic and anatomic images obtained form PET and CT scans and providing the clinicians with fusion images (Fig. 5). Whether integrated PET/CT scans substantially improve the accuracy of imaging in patients with lung cancer is the subject of many investigations.

Integrated positron emission tomography/computed tomography scan demonstrating cancer in the left lung with chest wall involvement and metastasis to left hilar and medistinal nodes and the left thoracic spine and ribs.
The accuracy of clinical staging in patients with stage I, II and III NSCLC, when compared with pathologic stage, is shown to be 68%, 84% and 74%, respectively.63 A recent study retrospectively evaluated the accuracy of integrated PET/CT scans in the staging of a suggestive lung lesion and compared the results with the accuracy of CT alone, PET alone and visually correlated PET/CT. Integrated PET/CT correctly predicted the tumour, node, metastasis (TNM) status and the stage in 86%, 80%, 98% and 70% of patients, respectively. The TNM status and the stage were correctly predicted in 68%, 66%, 88% and 46% of patients, respectively, with CT alone; 46%, 70%, 96% and 30% of patients, respectively, with PET alone; and 72%, 68%, 96% and 54% of patients, respectively with visually correlated PET/CT.64 Other studies have also reported similar findings, concluding that integrated PET/CT is more accurate than PET alone, CT alone or visually correlated PET/CT in tumour staging, node staging and detection of metastases.65–67
In evaluating the recurrence of NSCLC, one study reported that the sensitivity, specificity and positive and negative predictive values of integrated PET/CT for diagnosis of recurrence were 96%, 82%, 89% and 93%, respectively, compared with 96%, 53%, 75% and 90%, respectively, for PET alone.68
Integrated PET/CT, therefore, has the potential to become the new standard approach to imaging in the diagnosis and management of patients with NSCLC. Whether this technology will replace current imaging modalities (i.e., CT scan alone, mediastinoscopy) is debatable.
Novel traces for PET
The accuracy of PET is a function of FDG, its radio-labelled molecular marker, whose specificity is less than ideal. In an attempt to increase this specificity, other markers are being investigated.69–72 New tracers that have shown promise in early clinical studies include 18F-fluorothymidine, a proliferation marker that might give better specificity in the assessment of SPNs or better accuracy in the evaluation of early response; 11C-Choline, a marker that looks at cell membrane synthesis; (99m)Tc-Annexin V, or Apomate, an apoptosis imaging agent that could be correlated with overall and progression-free survival in phase I data; and 18F-fluoromisonidazole, which can be used to quantify regional hypoxia in human tumours using PET.73,74 However, to date, none of these tracers under development has proved superior to FDG in published data and no tumour-specific radiotracer for NSCLC has been identified. The development of such a marker would greatly improve the accuracy of PET imaging in the management of NSCLC.
Radiation treatment planning
The potential functional enhancement by PET combined with future advances in integrated PET/CT scans may also play an important role in radiotherapy treatment planning75 and in targeted molecular therapy of NSCLC.73 Another development that has shown a potential role in the management of NSCLC is virtual bronchoscopy using data sets from PET/CT. Data with this technology have been limited but are encouraging.76
The use of PET in radiation treatment planning may lead to further changes in patient management owing to upstaging the extent of disease, changing treatment intent from radical radiation to palliative treatment, increasing the radiation field size owing to the finding of unsuspected mediastinal node involvement not seen on CT scans, decreasing the treatment field size owing to better localization of the tumour in areas of associated atelectasis or post-obstructive pneumonitis77,78 and decreasing interobserver variation in target definition.79,80
Canadian clinical trials involving FDG-PET
In the United States, the Centers for Medicare and Medic-aid Services have approved reimbursement for PET use in staging and restaging of NSCLC. In Canada, no national policy has been adopted with regard to health care coverage of the cost of PET in the management of NSCLC. The Ontario PET scan trials, ELPET and PET START, are prospective randomized clinical trials currently underway. These trials collectively are designed to assess the application of PET in the staging of NSCLC, its effect on overall survival, the prognostic factor of SUV of the index lesion before treatment, accuracy of mediastinal staging and cost-effectiveness of PET use. It is hoped that the outcomes of these trials would further define the role of PET in the management of NSCLC and facilitate the determination of optimal therapy for this prevalent cancer.
Conclusion
We have shown the potential applications of FDG-PET in patients with NSCLC. Positron emission tomography is a potentially powerful imaging technology, and clinicians need to determine how best to integrate this tool in the management of NSCLC to improve patient outcomes while maintaining the financial integrity of health care systems.
Footnotes
Competing interests: None declared.
Contributors: Drs. Behzadi, Ung and Deschamps designed the review. Drs. Behzadi and Lowe acquired data, which Dr. Deschamps analyzed. Drs. Behzadi and Ung wrote the article, which Drs. Lowe and Deschamps reviewed. All authors gave final approval for publication.
- Accepted February 5, 2008.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.