


Abstract
Background: We sought to identify criteria for the intraoperative assessment of sentinel lymph node (SLN) involvement in women with early breast cancer. We also sought to determine whether the SLN nomogram developed by the Memorial Sloan-Kettering Cancer Center (MSKCC) to predict nonsentinel lymph node (NSLN) involvement when the SLN is positive would accurately predict NSLN involvement in our patient population.
Methods: We performed 405 SLN biopsies in 397 women between January 1998 and June 2005. We determined factors associated with SLN metastases using univariate and multivariate logistic regression. Ninety women who had 1 positive SLN or more and underwent axillary lymph node dissection (ALND) had complete data for analysis. We applied the MSKCC nomogram retrospectively to this subset of women, and we calculated the probability of NSLN involvement and compared it with the observed rate.
Results: Multifocality and the presence of lymphovascular invasion were predictive of SLN involvement. Ductal carcinoma in situ was negatively associated with SLN involvement. Intraoperative evaluation identified 57 (63%) of the 90 women with involved SLN, of which 26 (29%) had involved NSLN. Application of the MSKCC nomogram to our data set produced an area under the receiver operator characteristic curve of 0.71. The nomogram tended to overestimate the probability of NSLN involvement in our population.
Conclusion: Lymphovascular invasion and multifocality were associated with SLN involvement. Women with small low-grade tumours may not require routine intraoperative evaluation of SLNs. The MSKCC nomogram appears to be most useful as a decision aid in selecting those women with an involved SLN in whom ALND may be omitted.
The morbidity of surgical treatment for many women with early stage breast cancer has been reduced with the adoption of breast-conserving surgery1 and sentinel lymph node biopsy (SLNB).2 Integration of SLNB into the surgical management of breast cancer in Canada has been limited by a number of factors, including lack of available resources in some areas and ongoing controversies surrounding the indications for its use and interpretation of the results.3
Sentinel lymph node biopsy has an inherent false-negative rate of 5%–10%4,5 that cannot be entirely eliminated, even with multiple sectioning of the sentinel lymph node (SLN).6 Although the false-negative rate of SLNB is higher than that of axillary lymph node dissection (ALND),7 the clinical significance of this difference is diminished by the frequent use of adjuvant systemic therapy in node-negative disease. Given the selection of lower-risk patients for SLNB, the rate of axillary recurrence following a negative SLNB is very low,8–11 even when surveillance imaging is added.12 This rate has been reported to be less than that in the population of women undergoing ALND.7 Thus concerns about axillary recurrence when the SLN is negative appear to be unfounded.
Many institutions conduct intraoperative assessments of SLNs to select patients for ALND. Such assessments are resource-intensive, often result in prolongation of the surgical procedure and infrequently result in a change in intraoperative management, since most SLNs are free of metastases. Even when SLNs are involved, the sensitivity of intraoperative assessment is only 60%–70%.13 Thus the lack of intraoperative assessments of SLNs need not be a barrier to SLNB and, in those institutions where such assessments are available, it may be cost-effective to identify a subgroup of patients with a low probability of SLN involvement in whom intraoperative SLN assessment could be avoided.
When the SLN is positive, however, current guidelines recommend ALND to prevent axillary recurrence.14 The proportion of involved lymph nodes in an ALND appears to be an important prognostic factor for survival,15 and the results of the ALND may be used to plan further adjuvant therapy.16 When the presence of axillary metastases is documented preoperatively, either clinically or by image-guided biopsy,17 SLNB may be omitted and ALND performed directly. Since most axillary metastases are not detected preoperatively, we were interested in determining those factors associated with a positive SLN.
More recently, the necessity of ALND for staging in all patients with metastases to a sentinel node has been questioned, particularly if such staging information will not alter treatment recommendations.18 Furthermore, nonsentinel lymph nodes (NSLNs) are free of disease in 30%–60% of patients in which the SLN is involved.19 Since one of the tenets of SLNB is that prophylactic removal of uninvolved axillary lymph nodes does not improve outcome, the value of ALND in women whose NSLNs are free of disease has been questioned. In such women, ALND is unlikely to have any diagnostic, prognostic or therapeutic value, yet will predictably result in additional morbidity.20,21 This has led to an interest in predicting the probability of involvement of NSLNs in individual patients. A nomogram developed by the Memorial Sloan-Kettering Cancer Center (MSKCC) uses tumour factors, SLN factors and the method of detection of SLN metastases to determine the likelihood of NSLN metastasis.22 This nomogram has been shown to be more accurate in predicting NSLN metastasis than clinician estimation using the same data.23 The nomogram has been validated in patient populations in The Netherlands,24 Australia25 and the United States.26,27
We conducted this study to assist in the development of institutional guidelines for the conduct of SLNB. In particular, we sought to develop criteria for the intraoperative assessment of SLNs and to determine whether we could identify a subset of women with positive SLNs who could avoid ALND. The specific objectives were 1) to identify the factors predictive of an involved SLN to guide the intraoperative assessment of SLNs and 2) to determine the accuracy of the MSKCC nomogram for prediction of involved NSLNs in our patient population.
Methods
We prospectively gathered data on the conduct and outcome of all SLNBs performed by 4 experienced breast surgeons at Sunnybrook and Women’s College Health Sciences Centre (Sunnybrook) between July 1998 and June 2005.
Surgical technique
We performed SLNB using 99mTc-labelled sulfur colloid and isosulfan blue. Briefly, we injected unfiltered 99mTclabelled sulfur colloid (1 mCi in 8 mL normal saline) peritumourally or in the subareolar region, and we injected 0.1 mCi in 0.05 mL normal saline intradermally 30 minutes to 4 hours preoperatively. We also injected 2–5 mL of isosulfan blue (Lymphazurin; United States Surgical) after induction of anesthesia. We massaged the breast for 5 minutes. We marked a zone of diffusion around the injection site and identified a hot spot using a gamma probe (Navigator; Johnson & Johnson). We defined sentinel nodes as nodes that contained 99mTc-labelled sulfur colloid and/or isosulfan blue or that were suspicious on palpation.
Pathological examination
We evaluated all sentinel nodes intraoperatively by touch prep or frozen section. After fixation, we sliced lymph nodes in 3-mm slices and embedded them in paraffin. We took 3 pairs of sections from each block at 50 μM intervals. We stained 1 of each pair with hematoxylin and eosin, and we stained the second for cytokeratin with the monoclonal anticytokeratin antibody (Clone CAM 5.2; BC Biosciences). We evaluated SLNs from 79 patients enrolled in the National Surgical Adjuvant Breast and Bowel Project B-32 protocol intraoperatively by touch prep; immunohistochemical staining for cytokeratin was performed only at the discretion of the pathologist after looking at the hematoxylin and eosin.
Variables
We collected data on patient age, tumour size, tumour type, nuclear grade, Bloom and Richardson grade, lymphovascular invasion, multifocality, estrogen receptor, progesterone receptor, Her2 neu overexpression, number of SLNs removed, number of SLNs positive, method of detection of SLN metastases and size of SLN metastases.
Statistical analysis
We compared patient or tumour characteristics between Sunnybrook and the MSKCC using a χ2 test. We determined factors predictive of a positive SLN by univariate and multivariate logistic regression. We considered factors that had a significance of p ≤ 0.15 in univariate models for entry into the multivariate model. We expressed odds ratios for each factor, and we set statistical significance at p = 0.05 for the multivariate model. To validate the MSKCC nomogram in the subset with a positive SLN, we recorded data to conform to the covariate structure of the nomogram. We used the online nomogram to estimate the probability of NSLN involvement. For both the derived multivariate model predicting the probability of SLN involvement and the nomogram predicting the probability of NSLN involvement in the subset of women with a positive SLN, we derived a receiver operating characteristic (ROC) curve from the resulting predicted values, and we calculated the area under the ROC curve using Hanley and McNeil’s W statistic.28 We also produced calibration curves22 and Hosmer and Lemeshow’s goodness-of-fit test29 for the multivariate model and the nomogram. We performed all analyses using SAS version 9.1.3 (SAS Institute Inc.).
Results
A total of 397 women, including 56 having mastectomies for extensive ductal carcinoma in situ, underwent 405 SLNBs during the study period. We retreived a median of 2 (interquartile range 1–3) SLNs for all women. The median and interquartile range was the same for those who had at least 1 positive SLN and those who had all negative SLNs. Descriptive characteristics of the study population can be found in Table 1. At least 1 SLN contained metastatic disease in 95 of 405 (23%) SLNBs performed; 92 of these women then underwent ALND. Three patients did not undergo ALND. One refused ALND even in the event of intraoperative detection of SLN metastases. One had 8 SLNs retrieved, 2 of which contained micrometastases identified on final pathology, thus we felt that ALND would add little to staging or local control and did not perform the procedure. There is no available information about why the third patient did not undergo ALND. One patient had extensive axillary involvement, and the SLNB was performed as part of the surgeon’s learning curve rather than as a diagnostic test — the nomogram was not intended or validated for such application and we excluded this patient from our analysis. Complete data were available for 90 of 91 remaining patients who underwent a SLNB followed by ALND.
Patient characteristics
Factors associated with SLN involvement
We performed univariate and multivariate analyses to determine factors predictive of SLN involvement (Table 2). We included factors significant or approaching significance on univariate analysis — grade (grade 2, p = 0.003; grade 3, p = 0.047), final pathology is ductal carcinoma in situ (p = 0.020), lymphovascular invasion (p < 0.001), multifocality (p = 0.036), age at surgery (per year, p = 0.13), tumour size (1–2 cm, p = 0.08; > 2 cm, p = 0.019) and number of SLNs (p = 0.06) — in our multivariate analysis. The exception was grade because it was highly correlated with lymphovascular invasion and multifocality (χ2, p = 0.004 and p < 0.001, respectively). Estrogen receptor, progesterone receptor and Her2 neu over-expression status and the year of diagnosis were nonsignificant on univariate analysis (data not shown). Ductal carcinoma in situ was negatively associated with SLN involvement (p = 0.038 on multivariate analysis), whereas multifocality (p = 0.023) and lymphovascular invasion (p < 0.001) were associated with higher rates of SLN involvement. In particular, lymphovascular invasion was highly significant: 12% of the patients without a positive SLN had lymphovascular invasion compared with 58% of the patients with a positive SLN. Age at surgery, tumour size and number of SLNs were not significant in the multivariate model.
Logistic regression of the probability of a positive sentinel node
We subsequently grouped patients into deciles based on the predicted probability of a positive SLN to compare the mean predicted probability of a positive SLN for each decile with the actual proportion of patients with positive SLNs (Table 3). Correlation between the predicted and actual probabilities (correlation coefficient = 0.99) was found to be present when analyzed in a calibration plot (Fig. 1). We calculated the sensitivity and specificity of the model for prediction of SLN involvement in our data set, and we produced an ROC curve (Fig. 2). The estimated area under the curve was 0.80 with a Hosmer and Lemeshow goodness-of-fit χ2 statistic of 3.0 (p8 = 0.94), indicating that the derived model fit the observed data well. Application of the model predicted a positive SLN in 24% of SLNBs, compared with the 23% that we observed.

A calibration plot comparing actual and predicted probabilities of a positive sentinel lymph node (SLN). Correlation coefficient = 0.99.
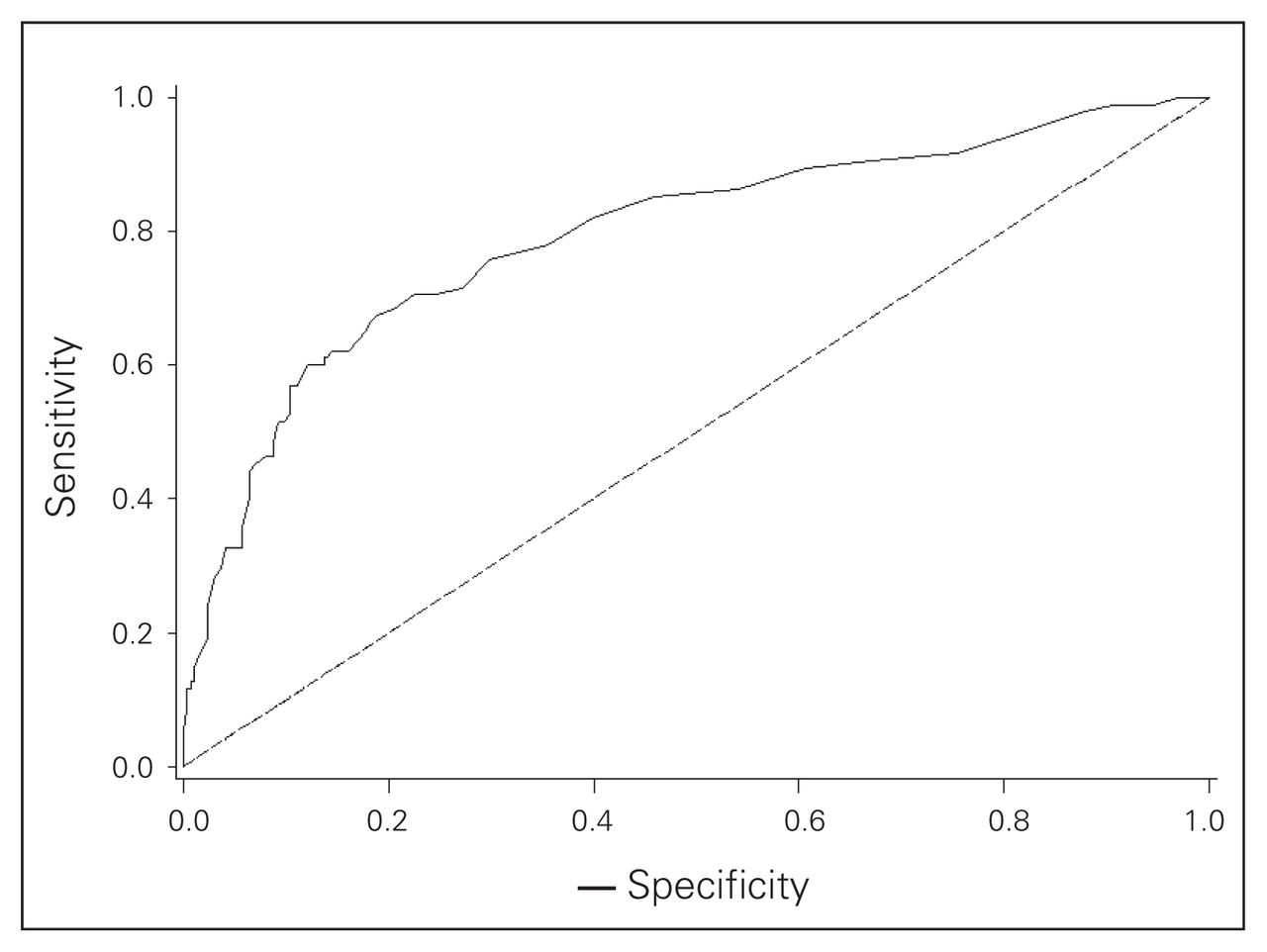
A receiver operating characteristic (ROC) curve assessing the model. The area under the ROC curve is 0.80.
Logistic regression of the probability of a positive sentinel node: actual versus predicted rate of sentinel lymph node involvement by deciles
Validation of the MSKCC nomogram
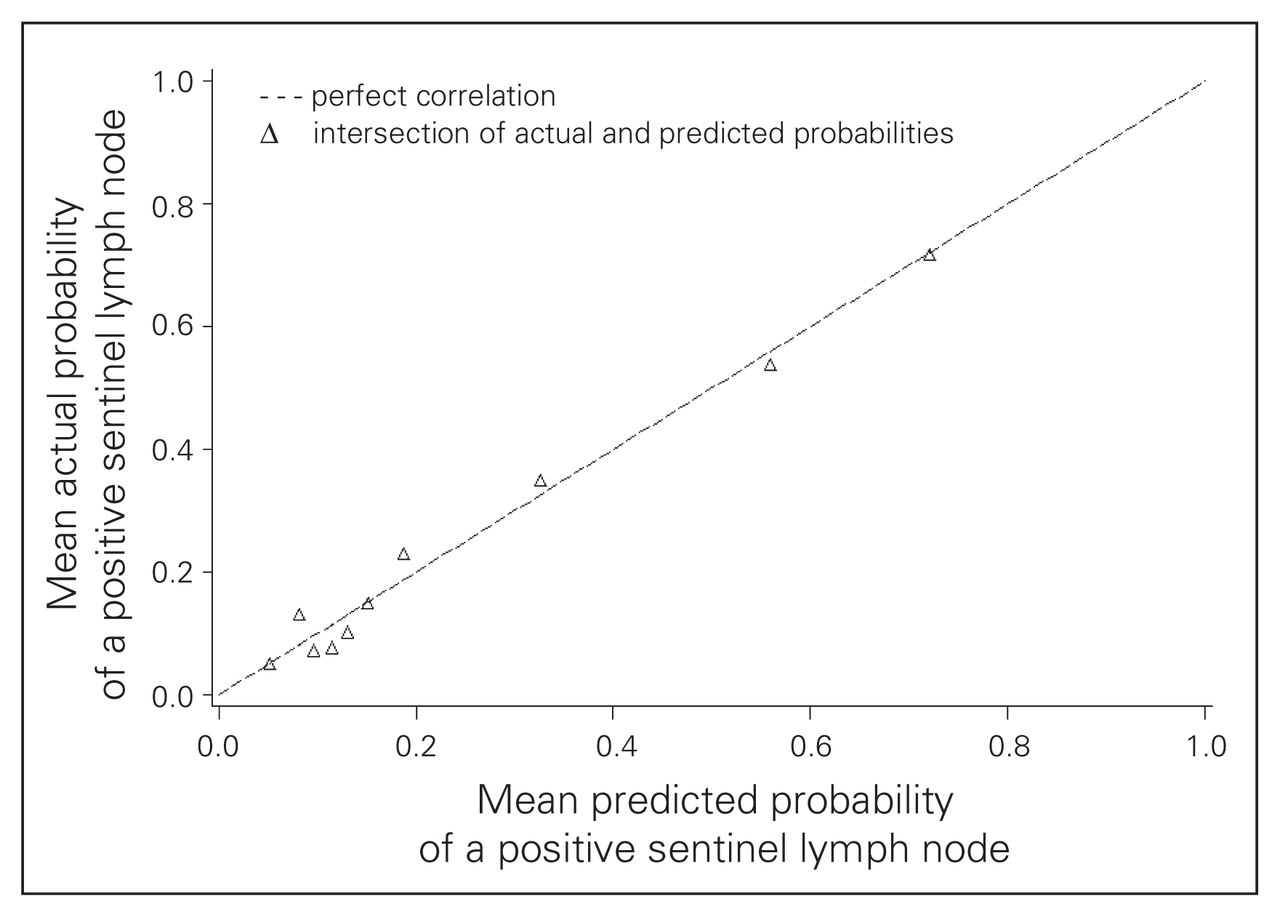
Compared with patients in the MSKCC population, our population with involved SLNs had some characteristics favouring a lower probability of NSLN involvement as predicted by the nomogram (Table 4). More of the Sunnybrook patients were Bloom and Richardson grade 1 (13% v. 3%), and fewer showed multifocality (18% v. 28%) or positive estrogen receptor status (71% v. 81%). In contrast, the presence of lymphovascular invasion was more frequent in the Sunnybrook cohort (58% v. 40%), and the absence of any uninvolved SLNs was also more frequent in the Sunnybrook cohort (50% v. 39%). There was a similar distribution of age, tumour size, number of positive SLNs and detection of SLN metastases by frozen section. We calculated the predicted probability of additional positive NSLNs using the MSKCC nomogram in the 90 patients with positive SLNs for whom complete data were available (nuclear grade was unavailable in 1 patient). The overall mean predicted probability was 38% (range 5%–95%), compared with the 29% of patients who actually had at least 1 positive NSLN. We grouped patients into deciles based on these predicted probabilities to compare the mean predicted probability of a positive NSLN for each decile with the actual proportion of patients with positive NSLNs (Table 5). Correlation between the predicted and actual probabilities (correlation coefficient = 0.74) was found to be present when analyzed in a calibration plot (Fig. 3). There was a tendency for the nomogram to over-predict NSLN involvement when compared with the actual data from the Sunnybrook population. We subsequently calculated the sensitivity and specificity of the nomogram for our data, producing an ROC curve (Fig. 4). The estimated area under the curve was 0.71 with a Hosmer and Lemeshow goodness-of-fit χ2 statistic of 15.1 (p8 = 0.60), indicating that the nomogram can reasonably predict but not closely fit the Sunnybrook data set.

A calibration plot comparing actual and predicted probabilities of a positive nonsentinel lymph node. Correlation coefficient = 0.74.
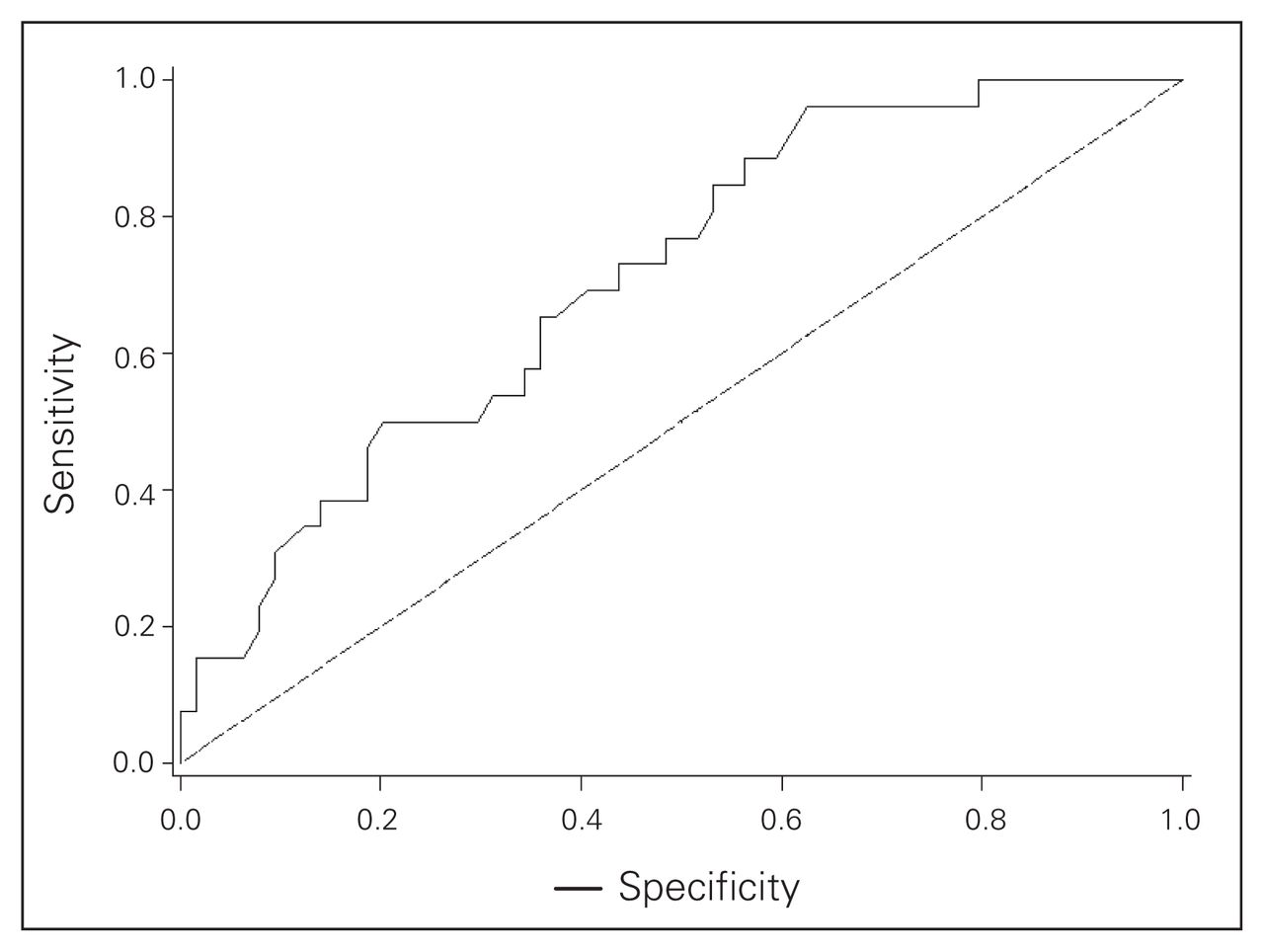
A receiver operating characteristic (ROC) curve assessing the nomogram. The area under the ROC curve is 0.71.
Comparison of tumour characteristics between the Sunnybrook and MSKCC patient populations with a positive sentinel lymph node
Application of MSKCC nomogram: actual versus predicted rate of nonsentinel lymph node involvement by deciles
We attempted to derive a nomogram for the prediction of NSLN involvement using our data, but although the direction of contribution of each variable in our derived model was the same as in the MSKCC model, the small number of patients precluded the development of a reliable model (data not shown).
Discussion
Our study showed that tumour grade 2 or 3, pure ductal carcinoma in situ, tumour size larger than 2 cm, lymphovascular invasion and multifocality were significantly associated with the probability of SLN involvement on univariate analysis (Table 2). These findings are similar to those of other groups.30–33 Ozmen and colleagues34 noted that patients whose tumours were associated with lymphovascular invasion were more likely to have positive SLNs on both univariate and multivariate analysis. Recently, Van den Eynden and colleagues35 determined that lymph vessel invasion and not blood vessel invasion was the only independent determinant of lymph node metastasis. Of these factors, only multifocality, lymphovascular invasion and a diagnosis of ductal carcinoma in situ were significant on multivariate analysis in our study (Table 3). The lack of significance for other covariates in the multivariate model may relate to the limited power of the data set, or the overwhelming effect of lymphovascular invasion as the dominant characteristic.
The multivariate model for prediction of SLN involvement fit closely with the data, and we were able to identify a population at low risk of SLN involvement who may not require routine intraoperative pathologic assessment of sentinel nodes. Women with small low-grade tumours are at low risk of SLN involvement, and these same factors also predict a low probability of NSLN involvement even if SLN metastases are present.22,36 Lymphovascular invasion often cannot be definitively determined to be absent on a core needle biopsy used for preoperative assessment, but as lymphovascular invasion was strongly correlated with grade in our study, selection of women with low-grade tumours may be a useful preoperative surrogate for those without lymphovascular invasion.
Ultrasound assessment of the axilla, with or without biopsy, is being increasingly used to identify women with axillary involvement preoperatively, thereby eliminating the need for SLNB before ALND.17,37,38 The specificity of this approach, reported as 73%–77%,17,37 is too low to warrant recommendation of axillary ultrasound as a substitute for SLNB. Most reported false-negative results on axillary ultrasound are generally associated with micrometastases,38 which similarly are associated with false-negative results on intra-operative assessment;39 thus axillary ultrasound may in future prove useful to guide selection of patients undergoing SLNB for intraoperative assessment. Currently, however, the technique itself is limited to specialized centres and is too operator-dependent to advocate a change in SLNB technique, including the use of intraoperative assessment, based on the results of preoperative axillary ultrasound examination. In contrast, we were unable to identify a group of women with a sufficiently high rate of SLN involvement to suggest that such women should not be offered SLNB. Although it would be reasonable to omit SLNB when the probability of the SLN being negative approached the false negative rate of SLNB, in our data set only 1% of patients had a 15% or less probability of a negative SLNB. The skewing of the data toward women with a lower probability of SLN involvement may be attributed to selective application of SLNB to lower-risk patients during the study period.
Although SLNB has been established as the procedure of choice for axillary staging among women who are node-negative, the risk of omitting completion ALND in women with an involved SLN has not been established in clinical trials. One trial comparing completion ALND versus axillary observation was closed owing to poor accrual (American College of Surgeons Oncology Group or ACOSOG Z0011 trial), whereas a phase III trial40 comparing ALND to axillary radiation is currently underway. Nonetheless, our current understanding of the biology of breast cancer is that prophylactic removal of uninvolved NSLNs is unlikely to have any direct therapeutic benefit. There is therefore considerable interest in decision aids to determine which women with positive SLNs are likely to benefit from ALND for residual disease.
We found that the MSKCC nomogram tended to over-predict NSLN involvement in our population. The area under the ROC curve was 0.71, which was lower than the value of 0.77 obtained when the nomogram was applied prospectively to the MSKCC population.22 Other groups that have undertaken the validation of the MSKCC nomogram within their patient population have calculated an area under the ROC curve of 0.72–0.86, suggesting our data are consistent with other published ROC curves.24–27
Use of immunohistochemistry for the evaluation of SLNs is widely used to minimize the risk of false-negative SLNBs, even if the significance of SLN metastases detectable only by immunohistochemistry remains controversial. Elimination of 12 patients in whom we detected SLN metastases with immunohistochemistry did not significantly alter the accuracy of the nomogram: the area under the curve was estimated at 0.70 with a 95% confidence interval of 0.57–0.83. The small difference in the area under the curve in our study compared with the MSKCC data may be related to differences in the underlying patient populations. Our population had a lower risk of NSLN involvement than the MSKCC population: the tumours tended to be of lower grade and more frequently unifocal and estrogen receptor–negative, all factors that predict a lower risk of NSLN involvement. In contrast, tumours in our data set more commonly had evidence of lymphovascular invasion, which has been associated with an increased risk of NSLN metastases in several studies.34,41–45 Although the area under the curve was reduced in our population compared with the MSKCC population, this does not directly relate to the clinical utility of the nomogram as reported by Degnim and colleagues.27 The reduction in accuracy of the nomogram in our population was predominantly related to a reduced specificity. As it was highly sensitive, application of the nomogram to our population would be more likely to result in ALND being performed when no NSLNs were involved, rather than omission of ALND in a significant proportion with residual axillary disease. Therefore, in our population with a low predicted probability of NSLN involvement, the risk of leaving residual disease is low. This finding contrasts the data of Kocsis and colleagues,46 who found that the nomogram underestimated the probability of NSLN involvement among low-risk women. With the threshold for performance of ALND set at a probability of NSLN involvement of 20%, the nomogram has 96% sensitivity in our population: in our cohort, 25 women, including 1 with NSLN involvement, would have been spared ALND. This analysis suggests a potential role for the MSKCC nomogram as a decision aid in our patient population, particularly if the predicted probability of NSLN involvement is low. As application of the nomogram requires information that is not available intraoperatively, selection of women with a low probability of SLN and NSLN involvement for ALND could await final pathologic examination with a low rate of repeat surgery. Decision analysis has shown that the use of intraoperative assessments of SLNs provides comparable quality of life to that associated with final pathologic assessment of the SLN.47 This implies that selective application of intraoperative assessment to those at greater risk of axillary disease may be a cost-effective strategy with little impact on patient satisfaction.
In conclusion, the presence of lymphovascular invasion and multifocality are associated with an increased risk of SLN involvement. Women with small low-grade tumours or ductal carcinoma in situ may not require intraoperative assessment of SLNs. The MSKCC nomogram tended to over-predict NSLN involvement in our population, suggesting that it would be most useful as a decision aid in selecting low-risk women in whom ALND may be omitted.
Footnotes
This work was presented at the 30th annual meeting of the American Society for Breast Disease, Las Vegas, Nevada, Apr. 27–29, 2006 (Abstract #2-19).
Competing interests: None declared.
Contributors: Drs. Quan and Holloway designed the study. Drs. Ramjeesingh, Quan and Holloway acquired and analyzed the data. Dr. Gardner also analyzed the data. Drs. Ramjeesingh, Gardner and Holloway wrote the article, which all authors reviewed and approved for publication.
- Accepted September 22, 2007.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.