


Abstract
Background: Regionalized approaches to trauma care improve patient outcomes. We developed and distributed a clinical reference poster to standardize the emergency department evaluation and management of patients with traumatic head injuries in hospitals throughout Nova Scotia.
Methods: We conducted a MEDLINE literature search to identify publications in the fields of prehospital and emergency management of head injuries. We reviewed and collated select studies to define contemporary standards of care.
Results: We derived a 3-tiered decision tool that summarizes the indications for resuscitation, radiography, specialty consultation and transfer of adult and pediatric patients with minor and major head injuries. A guideline poster was constructed and distributed to all provincial emergency departments upon approval by local trauma and critical care staff.
Conclusions: This report describes the evidence for a population-based, province-wide assessment and early management tool that was developed for health care personnel who treat patients with head traumas. Comparison of outcome data from preand postguideline eras will ultimately shed light on the use of regionalized approaches to managing brain injuries.
Regionalized emergency health services may contribute to improved clinical outcomes after traumatic brain injuries (TBIs) by providing standardized and more efficient acute care within a designated catchment area. Patients with head injuries who are assessed in the field or in the emergency department require accurate risk stratification to make management decisions that prevent secondary brain injuries.1–4 Occult lesions and delayed intracranial complications have been reported in up to 17% of people with apparently trivial head injuries, emphasizing the significance of a structured evaluation of these patients at initial presentation.5 In contrast, the need for aggressive resuscitation and intensive care monitoring is often quickly recognized after severe TBI; however, important issues regarding the timing and nature of the resuscitative efforts, as well as the urgency of patient transport and neurosurgical consultation, may be poorly defined.5–10 Standardized algorithms and clinical predictors of intracranial11,12 or cervical spine13,14 injury have been reported and validated, yet the impact of regionalized TBI care on patient outcomes remains unknown. To our knowledge, there have been no clinical decision tools published that provide a comprehensive approach, based on the current state of knowledge, to the acute care of adult and pediatric patients who present to the emergency department with head injuries.
Trauma services in Nova Scotia are coordinated through a regionalized system that serves a population of 940 000 in an area of 53 000 km2 (20 463 square miles). A single neurosurgical service operates at adult and pediatric tertiary care centres located in Halifax and receives all major neurotrauma patients in the province. Ground and air ambulance activity is organized by a central dispatchment unit that is accessible province-wide via a 24-hour trauma hotline. In optimal conditions, each municipality is within 90 minutes travel by helicopter from Halifax, and all efforts are made to transport patients, by ground or air, immediately to the most appropriate hospital. The role of the neurosurgical service within this type of health system is ideal for assessing the impact of regionalized protocols in the management of acute head trauma. In this report, we present evidence for a novel reference guide that was developed as part of a population-based initiative to standardize the care of adult and pediatric patients with head injuries who present to emergency departments throughout Nova Scotia.
Materials and methods
We conducted a MEDLINE review of the literature between 1970 and 2005, using the primary medical subject headings “head injury” and “management.” Searches were culled to identify articles regarding prehospital, emergency department and intensive care of TBI patients, as well as guideline publications and review articles that addressed regionalized approaches to trauma and TBI management. Current recommendations included those founded by multiple clinical groups, substantiated by long-term conventional applications, and supported by a well-designed cohort or randomized trials. This instrument is intended to facilitate the management of traumatic head injuries in the emergency department and, apart from resuscitative measures, does not provide recommendations regarding prehospital or definitive care. After consultation with the provincial trauma and critical care communities, we distributed this guideline to all emergency departments throughout Nova Scotia.
Results
Initial neurological evaluation
It is useful to categorize patients with head injuries according to their age and presenting Glasgow Coma Scale (GCS) score, because both of these parameters influence management and prognosis (Box 1). The GCS score remains the most widely used measure of neurological function in TBI patients and has significant prognostic value when graded in the absence of sedation, chemical paralysis or intoxication.15–19 The GCS has high inter- and intraobserver reliability and has been used to arbitrarily define injury severity as mild (GCS score 13–15), moderate (GCS score 9–12) or severe (GCS score 3–8). Because the acute management of moderate and severe head trauma is comparable, the current recommendations are based on the simpler dichotomy of minor (GCS 13–15) and major (GCS 3–12) categories. The pediatric GCS that is included in the guideline is a modified version of the original scale and is one of several triage-scoring systems adapted for children.20,21
Glasgow Coma Scale (GCS)*†
| Modality | Score | Adult | Pediatric |
|---|---|---|---|
| Eye opening (E) | 4 | Spontaneous | Spontaneous |
| 3 | To speech | To speech | |
| 2 | To pain | To pain | |
| 1 | None | None | |
| Verbal (V) | 5 | Oriented | Appropriate for age; fixes and follows sensory cues; social smile |
| 4 | Confused | Cries, but consolable | |
| 3 | Inappropriate | Persistently irritable | |
| 2 | Incomprehensible | Restless, lethargic | |
| 1 | None | None | |
| Motor (M) | 6 | Obeys commands | Spontaneous |
| 5 | Localizes to painful stimuli | Localizes to painful stimuli | |
| 4 | Withdraws from pain | Withdraws from pain | |
| 3 | Abnormal flexion (decorticate) | Abnormal flexion (decorticate) | |
| 2 | Abnormal extension (decerebrate) | Abnormal extension (decerebrate) | |
| 1 | None | None | |
Minor head injuries (GCS 13–15) in adult patients
Minor head injuries are associated with a brief loss of consciousness, disorientation or amnesia in patients with a GCS score of 13 to 15.15,22,23 Most patients are stable at the time of examination, and it is important to recognize those at risk of occult or evolving intracranial lesions. Several groups have attempted to identify reliable indicators of intracranial injury and the need for urgent CT.11,12,24,25 The Canadian CT Head Rule predicts the need for neurological intervention with a sensitivity of 100% and a 95% confidence interval between 92% and 100%.12,26 The 3-year study data were compiled from 3121 adult patients in 10 Canadian centres and identified 5 clinical signs that have previously been associated with TBI. Patients with minor head injuries and evidence of prolonged GCS impairment,23,27–29 depressed skull fracture,28,30,31 basal skull fracture, 28,32 recurrent vomiting33,34 or age 65 years or over2,30 are at high risk of requiring neurological treatment and should have urgent CT imaging. Although a normal CT scan does not preclude latent hemorrhage, the incidence of significant deterioration in these patients is exceedingly low and justifies chaperoned discharge when clinically well.35 In contrast, radiographic evidence of intracranial injury warrants a neurosurgical consultation. If the patient is being evaluated in a tertiary care centre, the neurosurgical housestaff should be contacted directly. However, if the emergency department encounter occurs in a nontertiary centre, the attending physician should immediately contact the local neurosurgeon on-call, which, in our system, may be accomplished by calling the Trauma Hotline. The neurosurgeon on-call is available to review the history (via telephone contact with the referring emergency department physician) and radiology (via viewing the CT scan on a province-wide real-time digital imaging system) and will provide advice regarding patient disposition and management (Box 2).
Approach to adults with minor head injuries*†
| CT urgently needed if all 3 of the following criteria are met12 |
| 1. History of blunt head trauma within past 24 h |
| 2. History of loss of consciousness, amnesia or disorientation |
| 3. One or more of the following risk factors present: |
| GCS score < 15 after 2 h after injury |
| Suspected open or depressed skull fracture |
| Signs of basal skull fracture |
| Recurrent vomiting |
| Age > 65 yr |
| Abnormal CT |
| Urgent neurosurgical consultation. |
| Normal CT or no CT indicated |
| Discharge when clinically well. Follow up with family doctor. |
GCS = Glasgow Coma Scale.
↵* GCS score 13–15.
↵† These patients are neurologically well but may be at risk of delayed complications. Indications for CT imaging and choice of disposition are the primary issues of acute care. Patients with a deteriorating GCS or penetrating head trauma are managed as a major head injury.
Minor head injuries (GCS 13–15) in pediatric patients
Children aged less than 2 years
Most pediatric head injuries do not require surgical intervention.36–39 Unusual or unexplained trauma in young children should raise a suspicion of abuse and be duly investigated. Those aged under 2 years require judicious management, because the growing calvarium and immature brain are susceptible to relatively low-impact forces.40–42 In addition, clinical signs of TBI are unreliable at this age, and neurological evaluation is hampered by limited verbal and behavioural repertoires.43,44 Any suggestion of TBI warrants further investigation, accepting that radiographic imaging may require sedation, with the associated risks of cardiovascular and respiratory complications.9,43,45,46
The highest incidence of skull fractures and intracranial injuries occurs in children aged under 1 year.47–49 Diagnosis of a skull fracture is important to ensure that clinical follow-up is arranged to monitor for the presence of a growing skull fracture. Scalp hematomas are a useful predictor of underlying fractures in young children, but up to 50% of asymptomatic patients will have skull or intracranial injuries without evidence of scalp trauma or neurological deficits.44,48,50–52 Therefore, it is recommended that children aged under 2 years undergo CT imaging if there is evidence of a neurological abnormality, such as decreased level of consciousness, nausea, lethargy or agitation. All asymptomatic children under age 1 year who present with a scalp hematoma require skull radiography and, if abnormal, a subsequent CT scan and neurosurgical consultation (Box 3).45,52–54
Approach to children with minor head injuries*†
| Age < 2 yr |
| Urgent CT head indicated if symptomatic (vomiting, lethargic, irritable) or neurologically abnormal. |
| If asymptomatic and neurologically normal, no further studies are required, except for children < 1 year with a scalp hematoma; then, obtain skull x-rays and CT head if plain radiography is abnormal. |
| Age 2 to 15 yr |
| Obtain CT head if GCS < 15. |
| If GCS = 15 and there is a history of loss of consciousness or posttraumatic amnesia, then either CT head or observe overnight. |
| If GCS = 15 with no history of loss of consciousness or posttraumatic amnesia, obtain CT head if ≥ 1 of the following are present: |
| Change in GCS score |
| Focal neurological deficit |
| Clinical evidence of skull fracture |
| Coagulopathy |
| All pediatric trauma patients with radiographic abnormalities of the head require urgent neurosurgical consultation. |
Children aged 2 to 15 years
Children in this age group with recent head trauma and a GCS score of 13 or 14 are at high risk of harbouring an intracranial lesion and require urgent CT imaging.55–57 Post-traumatic amnesia and loss of consciousness have traditionally been considered risk factors for TBI; however, there are no prospective studies that have identified one or more clinical signs that accurately predict intracranial abnormalities.9,39,51,58,59 The guidelines published by the American Academy of Pediatrics recommend either observation or CT scanning for neurologically normal (i.e., GCS score of 15) children who have experienced loss of consciousness and recommend observation only for those who have not.7 More recent guidelines favour CT studies for children with amnesia, a history of loss of consciousness, impaired mental status, focal neurological deficits, evidence of skull fracture or coagulopathy. 60 Children who meet the criteria for an urgent CT, and where the CT is abnormal, require prompt neurosurgical consultation (Box 3).
Major head injuries (GCS 3–12) in adult and pediatric patients
Standard trauma guidelines recommend that patients with major head injuries receive aggressive cardiopulmonary and hemodynamic resuscitation unless an obvious reason exists to withhold treatment.61 Cervical spine fractures and systemic injuries are present in 6% to 8% and 50% of these patients, respectively, and must be considered during the resuscitative phase of treatment.62–64 The incidence of secondary brain injuries can be significantly reduced by prevention of hypoxia, hypotension and elevated intracranial pressure (ICP). Maintenance of a cerebral perfusion pressure 70 mm Hg or greater may reduce TBI mortality and, in the absence of marked ICP elevation, can usually be achieved with a mean arterial blood pressure of 90 mm Hg.6 Intracranial hypertension develops in 40% of patients with severe TBI and may be associated with anisocoria, papilledema, neurological deficits or a deteriorating level of consciousness.65 Valsalva manoeuvres produced by cough, movement or pain elevate ICP and often require suppression with narcotics, sedatives or paralytic agents. Osmotic diuretics (e.g., mannitol) and hyperventilation reduce ICP, in part, by decreasing cerebral interstitial and intravascular volumes, respectively. 6,66,67 These measures require prudent monitoring and fluid management, because subsequent hypovolemia and hypocarbia may exacerbate cerebral ischemia.68,69 Brief periods of hyperventilation are currently reserved for use in acute herniation syndromes with brainstem compromise. If the ICP cannot be controlled with medical management, invasive procedures such as ventricular drain placement or decompressive craniectomy may be considered by the attending neurosurgeon.
If a patient with severe TBI is being evaluated at the scene or requires resuscitation at a peripheral hospital, the immediate goals should be cardiopulmonary and hemodynamic stabilization followed by prompt transfer to a neurosurgical centre. Investigations that are not directly related to resuscitative efforts should be postponed until the patient has reached definitive care. Delayed treatment significantly impacts clinical outcome, and the mortality of specific intracranial lesions may be reduced by as much as 66% if patients receive surgery within 4 hours of injury.8,70–72 Referring physicians should rapidly assess and stabilize patients while maintaining spinal precautions and monitoring for acute neurological changes. A brief (2-minute) assessment of the GCS score, pupillary responses, deep tendon reflexes and gross motor function provides a neurological synopsis for the receiving trauma team and facilitates monitoring during patient transfer (Box 4).
Approach to patients with major head injuries*†
| Advanced trauma life support |
| Intubation required for GCS ≤8 or deteriorating level of consciousness; oxygen by mask for others |
| Global clinical assessment |
| Prevention of hypoxia and hypotension |
| Maintenance of spinal precautions at all times |
| Brief neurological examination |
| GCS score |
| Pupil size and reactivity |
| Deep tendon reflexes |
| Babinski response |
| Gross motor function |
| Urgent transfer to a neurosurgical service |
GCS = Glasgow Coma Scale.
↵* GCS score 3–12.
↵† Resuscitation and transfer to a neurosurgical service should be the priority of acute care. Spinal and systemic injuries are commonly associated and must be considered during treatment. A brief neurological examination provides valuable clinical information for monitoring and assessment by the receiving physicians, particularly if performed before the administration of sedatives or paralytic agents.
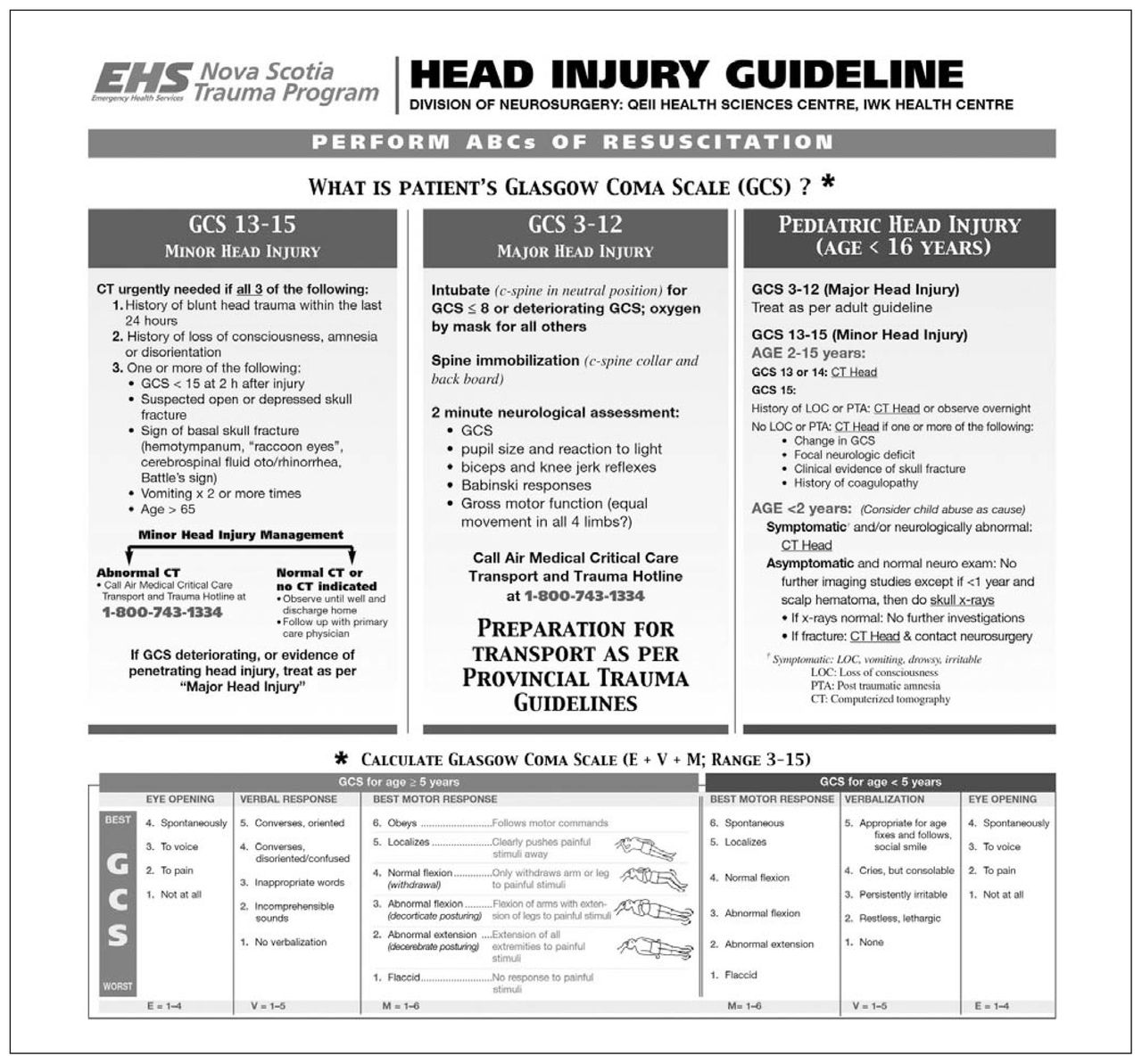
The recommendations outlined above for the assessment and acute care of adult and pediatric patients with TBI have been collated into a single guideline poster that has been displayed in the emergency department of each of the 8 district health centres throughout Nova Scotia (Fig. 1). These 8 centres represent all the regional hospitals that see most of the nontertiary care head injuries in the entire province and, thus, are immediately served by this clinical guideline. A recent survey of the emergency medicine department chiefs for these regional hospitals was conducted (December 2005–January 2006). The survey was constructed with a modified Dillman technique; a copy of the survey is available from the authors on request.73 Surveys were mailed out with a self-addressed envelope, and subsequent telephone follow-up was performed twice. With the small number of subjects (8), the response rate was 100%. The survey results show that the guideline is currently being used at each centre and is posted in all 8 emergency departments. The survey also demonstrates that the guideline has been “beneficial to the management of TBI patients” (100% response) and has led to modifications in local practice, such as CT imaging, earlier patient transfer or both in 50% of the regional centres.
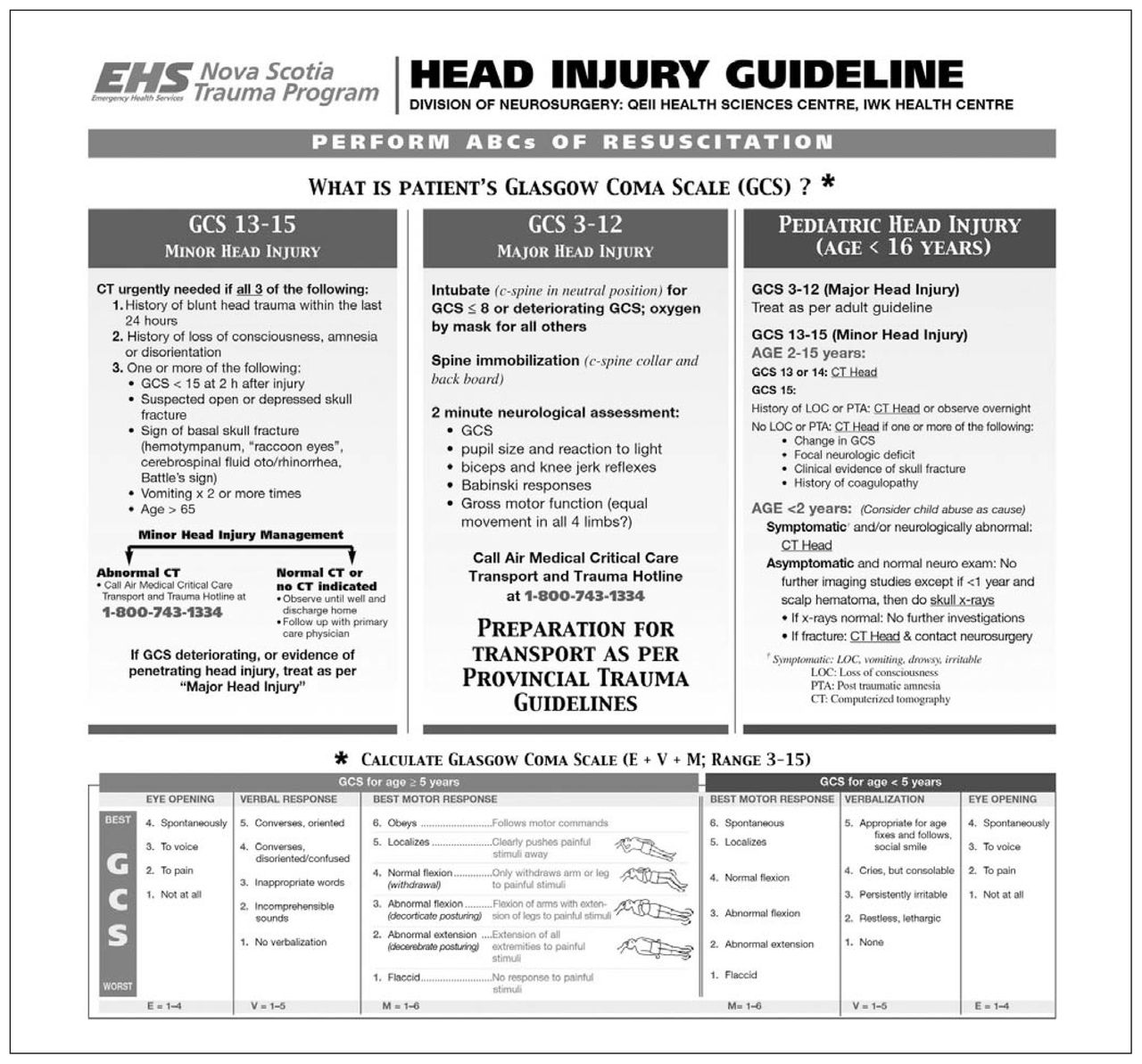
The Nova Scotia Head Injury Guideline. The telephone numbers and directives for specific transport protocols displayed on the poster are not generalizable to other geographic regions.
Discussion
Injuries are the largest contributor to mortality in people aged under 40 years and represent the fourth overall cause of death in North America.74–77 The annual incidence of TBI in the United States has been estimated between 100 and 367 per 100 000 population, and billions of dollars are spent each year on medical, social and rehabilitation services.6,78,79 The high incidence of TBI in young adults contributes to an enormous loss of potential life years, with the American prevalence between 2.5 and 6.5 million individuals.79 In Canada, population- based data are limited; nonetheless, approximately 18 000 patients are admitted to hospital annually for head injuries, and regional incidences have been reported at 16 and 7 per 10 000 per year in male and female patients, respectively (Kingston, Ontario) 80 and 14 per 10 000 population per year aged over 16 years (Nova Scotia).81 A 4-year review in eastern Ontario revealed that closed head injuries produce some of the most common and severe anatomic lesions in pediatric trauma.82 Thus, the social and economic impact of head trauma in North America is substantial and provides the impetus for ongoing research into clinical prevention, management and repair strategies. Trauma system regionalization has resulted in more efficient patient management and improved clinical outcomes following systemic injuries.72,83–86 The development and promotion of evidence- based treatment guidelines and decision rules also facilitate injury assessment, resuscitation and patient disposition.87–89 Unfortunately, although there are limited studies that suggest that implementation of treatment protocols may also benefit TBI patients, many aspects of TBI care remain without objective support and current medical practices vary according to regional experiences and resource availability.90–92
Conclusions
Head trauma produces a wide spectrum of injury and requires proficient early management to detect occult lesions and prevent secondary cerebral insults. We have created and disseminated a novel reference guide, based on the current state of knowledge, as part of an initiative to standardize the assessment and early management of TBI in Nova Scotia. This instrument may be easily modified for other geographical regions. Its implementation is expected to improve patient outcomes by facilitating management decisions in the emergency department and expediting the transfer of appropriate individuals to neurosurgical expertise.
Footnotes
This work was presented in abstract and poster format at the 2004 Annual Meeting of the American Association of Neurological Surgeons.
Competing interests: None declared.
- Accepted February 16, 2006.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.