


Abstract
Introduction: To review the circumstances surrounding the misdiagnosis of transient osteoporosis of the hip (TOH) as avascular necrosis (AVN) and to increase physician awareness of the prevalence and diagnosis of this condition in young men, we reviewed a series of cases seen in the orthopedic unit at St. Michael’s Hospital, University of Toronto.
Methods: We studied the charts of patients with TOH referred between 1998 and 2001 with a diagnosis of AVN for demographic data, risk factors, imaging results and outcomes.
Results: Twelve hips in 10 young men (mean age 41 yr, range from 32–55 yr) were identified. Nine men underwent magnetic resonance imaging (MRI) before referral, which showed characteristic changes of TOH. All 10 patients were referred for surgical intervention for a diagnosis of AVN. The correct diagnosis was made after reviewing patients’ charts and the scans and was confirmed by spontaneous resolution of both symptoms and MRI findings an average of 5.5 months and 7.5 months, respectively, after consultation.
Conclusions: Despite recent publications, the prevalence of TOH among young men is still overlooked and the distinctive MRI appearance still misinterpreted. Symptoms may be severe but resolve over time with reduced weight bearing. The absence of focal changes on MRI is highly suggestive of a transient lesion. A greater level of awareness of this condition is needed to differentiate TOH from AVN, avoiding unnecessary surgery and ensuring appropriate treatment.
Transient osteoporosis of the hip (TOH) was first described by Curtiss and Kincaid in 19591 as a syndrome of transient demineralization of the hip in the third trimester of pregnancy. In 1968, Lequesne2 first used the term in a published report. This rare cause of acute hip pain is still a relatively unknown clinical entity.
Characteristically, this skeletal disorder is a distinct self-limiting condition that presents spontaneously with sudden-onset pain in the hip, gradually resolving within 6–8 months.3–6 No intervention is needed for this condition, and management essentially involves symptomatic relief and avoiding excessive activity to minimize the risk of a pathologic fracture until the osteoporosis resolves.3
Unlike TOH, avascular necrosis (AVN) is a progressive condition, resulting from an interruption of the tenuous vascular supply to the femoral head. AVN is a more common cause of acute hip pain than TOH, and early surgical intervention may prevent further deformity of the hip joint.7 Although the prognosis and treatment of these 2 conditions differ greatly, in the early stages the radiographic appearance of TOH may be confused with AVN,8 resulting in unnecessary operative intervention with its accompanying risks and consequences. It is, therefore, vital to distinguish TOH from AVN early in its clinical course.
Several studies have investigated the best means to differentiate TOH and AVN. Radiographs lack sensitivity for TOH as osteopenia is only evident 4–8 weeks after the onset of symptoms,9 and although bone scans are sensitive, the positive result of homogeneous increased uptake is not specific for TOH.4 To date, the most reliable investigation for this purpose has been magnetic resonance imaging (MRI)10,11 with abnormalities consistent with TOH reported within 48 hours of onset of symptoms.12
TOH is commonly considered in acute hip pain in pregnancy, but its occurrence in middle-aged men is less well recognized, and is actually far more common in young to middle-aged men.3 In this study we describe the clinical features and course of the disease in 10 young adult men with TOH referred to the orthopedic unit at St. Michael’s Hospital, Toronto, for operation after a misdiagnosis of AVN. Our aim is to increase awareness of this condition in middle-aged men. In addition, we will attempt to define the clinical and radiologic characteristics that distinguish AVN from TOH to ensure appropriate treatment of these men in the future.
Patients and methods
Our university-affiliated tertiary-care orthopedic unit specializes in femoral head-sparing procedures in patients with AVN of the hip. Thus, this population represents a select group of patients who are younger (age < 60 yr) and have earlier stages of the condition (Steinberg stage IV or less)7 than an average group of patients with AVN. Between 1998 and 2001, 196 patients were patients referred for surgical intervention with a diagnosis of AVN of the hip. All were seen and evaluated by a single orthopedic consultant (M.D.M.). The findings of plain radiography and MRI were reviewed by a consultant radiologist (D.P.).
From this group, we identified 10 men (12 hips) who had clinical and radiographic findings consistent with TOH. All 10 had undergone plain radiography and MRI of the involved hip(s). All had had an original referring diagnosis of AVN of the femoral head. None had undergone surgery on the involved hip that would affect the MRI results. These patient records were reviewed by an independent examiner (A.B.), and information was obtained on age, sex, risk factors for TOH or AVN, radiographic, bone scan and MRI findings, as well as relevant medical history and outcomes.
Results
The mean age of these patients was 41.0 years (range from 32–55 yr, Table 1). In 5 of these patients the right hip was affected, in 3 patients the left hip was affected, and in 2 patients both hips were affected sequentially. The average duration of symptoms before the patients were seen at this institution was 4.7 months (range from 2–8 mo).
Demographic Data, Symptoms and Physical Findings in 10 Patients With Transient Osteonecrosis of the Hip
Radiography was performed on all patients (Table 2). Six patients had no radiographic changes, and in 4 patients the only change was diffuse osteopenia of the affected femoral head and periarticular acetabular bone, noted an average of 2.5 months (range from 2–3 mo) after the onset of symptoms (Fig. 1). In 2 cases (nos. 5 and 6) in whom TOH was bilateral, radiography and bone scanning were not done for the second affected hip, and MRI was used as the initial imaging modality.

Plain radiograph of transient osteoporosis of the left hip. Osteoporosis of the left femoral head and neck as well as periacetabular osteopenia can be seen. The right hip is normal.
Summary of Abnormalities Found on Radiography, Magnetic Resonance Imaging and Bone Scanning in 10 Patients With Transient Osteonecrosis of the Hip*
Bone scanning was done in 9 patients and all showed uniformly increased uptake at the affected femoral head extending down into the femoral neck and intertrochanteric region.
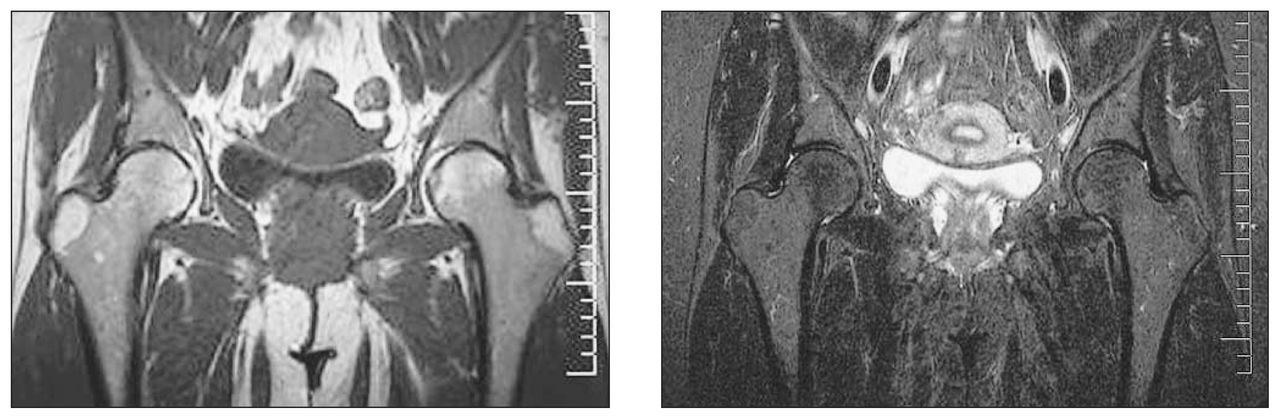
Each patient underwent MRI. The characteristic changes of TOH on MRI, seen in all our patients, are a pattern of diffuse edema, the absence of focal defects, an intact articular surface and the absence of a double line sign, usually associated with a joint effusion. The diffuse edema pattern was identified by a homogeneously decreased signal on T1-weighted images and a homogeneously increased signal on fat-suppressed T2-weighted images, extending from the superior articular surface of the femoral head to the femoral neck and intertrochanteric region (Fig. 2). The extent of edema in TOH usually exceeds the amount that would be expected in AVN.10 In our patients, these images were initially misinterpreted as showing changes consistent with AVN.

A coronal T1-weighted magnetic resonance image of both hips (left) shows diffiuse low signal intensity throughout the left femoral head and neck. A corresponding coronal T2-weighted image with fat saturation (right) shows diffuse high signal intensity in the left femoral head and neck with a joint effusion. These findings are typical of transient osteoporosis of the left hip.
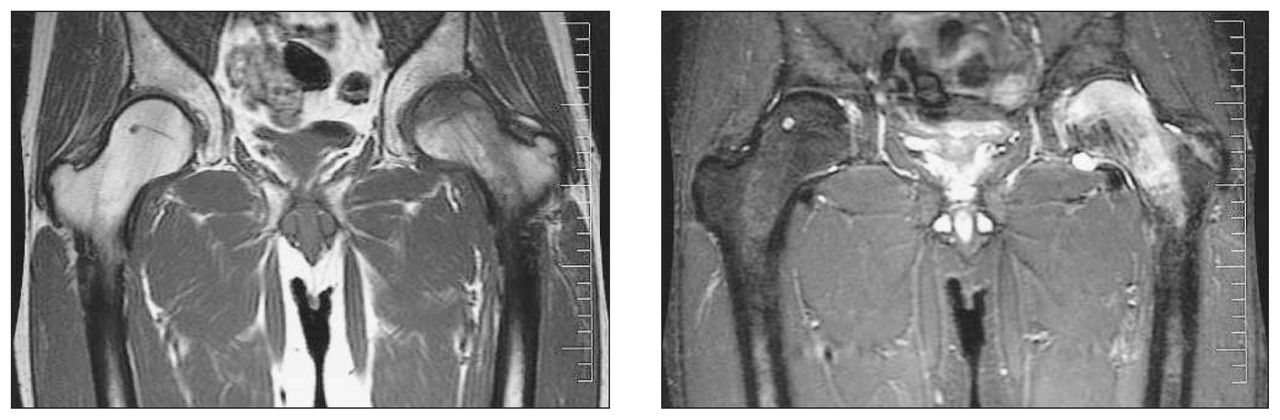
The time taken for complete resolution of the MRI changes averaged 7.5 months (range from 4–11 mo) (Fig. 3). No patient had any evidence of femoral head collapse or change in sphericity on follow-up MRI. Follow-up MRI was not done in 2 of the 12 hips (2 patients). Both lived in northern Ontario where there was no access to an MRI scanner locally. Both were contacted and reported complete resolution of hip symptoms. Neither would return for repeat MRI.
A coronal T1-weighted image (left) and a T2-weighted image (right) obtained 4 months after a diagnosis of transient osteoporosis of the left hip by magnetic resonance imaging shows complete resolution of the previous low T1 and high T2 signal intensity in the femoral head and neck. A previously noted effusion has resolved.
All patients were managed conservatively. This included advice to avoid excessive activities to minimize the risk of pathologic fracture and the administration of anti-inflammatory agents for symptomatic relief. The average time to spontaneous resolution of symptoms was 5.8 months (range from 2–10 mo, Fig. 4).

The time to resolution of symptoms in each of the 10 patients with transient osteoporosis of the hip (TOH). Cases 5 and 6 had TOH in both hips, so the time taken for the osteoporosis in both hips to resolve has been averaged and this average is represented on the graph. In case 5 the symptoms resolved in 6 months for the left hip and 5 months for the right hip, whereas in case 6, the time taken was 6 months for both sides.
Discussion
TOH is classically associated with pregnancy, but is often seen in young men, as in our series. Three of the 10 patients in this series and 24 of 56 patients in a previous series3 reported experiencing rest pain or night pain, features considered far more typical of AVN. This may have been one of the reasons for the misdiagnosis of the patients in this series (Table 1). The pain resolved spontaneously over time with reduced weight bearing; in contrast AVN would be expected to cause progressive, intractable rest and night pain.
Patients 1 and 4 both sustained an episode of minor trauma preceding their hip pain, which may have caused a period of transient ischemia precipitating TOH.13 This history of trauma may also have confused the diagnosis as the acute hip pain was initially attributed to a muscle strain, and patient 1 had been experiencing hip pain for 8 months before a referral was made to the orthopedic specialist.
Patients 3 and 6 were both hypothyroid on thyroxine supplements. Premenopausal women on thyroxine supplements have lower bone density at the femoral neck and trochanter than women without thyroid disease,14 and iatrogenic hyperthyroxinemia may cause decreased bone density at doses that will not cause clinical hyperthyroidism. 15 Neither patient reported symptoms of thyrotoxicosis or had recent abnormal thyroid function. No association has been shown between thyroid dysfunction and AVN. Patient 7 was on daily coumadin treatment following a cerebrovascular accident 6 years previously. Coumadin has been shown to provide pain relief in osteonecrosis of the jaw,16 but no data have been presented on its therapeutic effect on AVN of the hip.
Two patients had known risk factors for AVN. Patient 10 had a long history of severe asthma that had necessitated the use of intermittent treatment with high-dose prednisone,17 and patient 7 had experienced idiopathic AVN of the left hip 10 years previously and had undergone surgical intervention. In retrospect, that diagnosis may be in question. Although some have reported a relationship (temporally) between TOH and AVN, we believe they are distinct entities, and we have not seen femoral head collapse or progression to arthritis in TOH patients. AVN has been reported to be bilateral in 50% of cases, and patient 7 was referred urgently before undergoing MRI.18 The correct diagnosis of TOH was confirmed on MRI at this institution.
Hence, with the exception of no. 7, all patients had MRI changes characteristic of TOH but were referred with a diagnosis of AVN. The diffuse edema pattern that occurs with TOH was of very low specificity and can also occur in AVN, but subchondral and focal abnormalities are specific to AVN19 (Figs. 5 and 6). Vande Berg and colleagues19 in their prospective study found that the absence of any subchondral changes on T1- or T2-weighted images had a 100% positive predictive value for transient lesions. The presence of a subchondral area of low signal intensity of at least 4 mm had an 85% positive predictive value on T2-weighted images and 87% on T1-weighted images for irreversible lesions.19 None of the 10 patients in our series had any focal or subchondral changes on MRI.

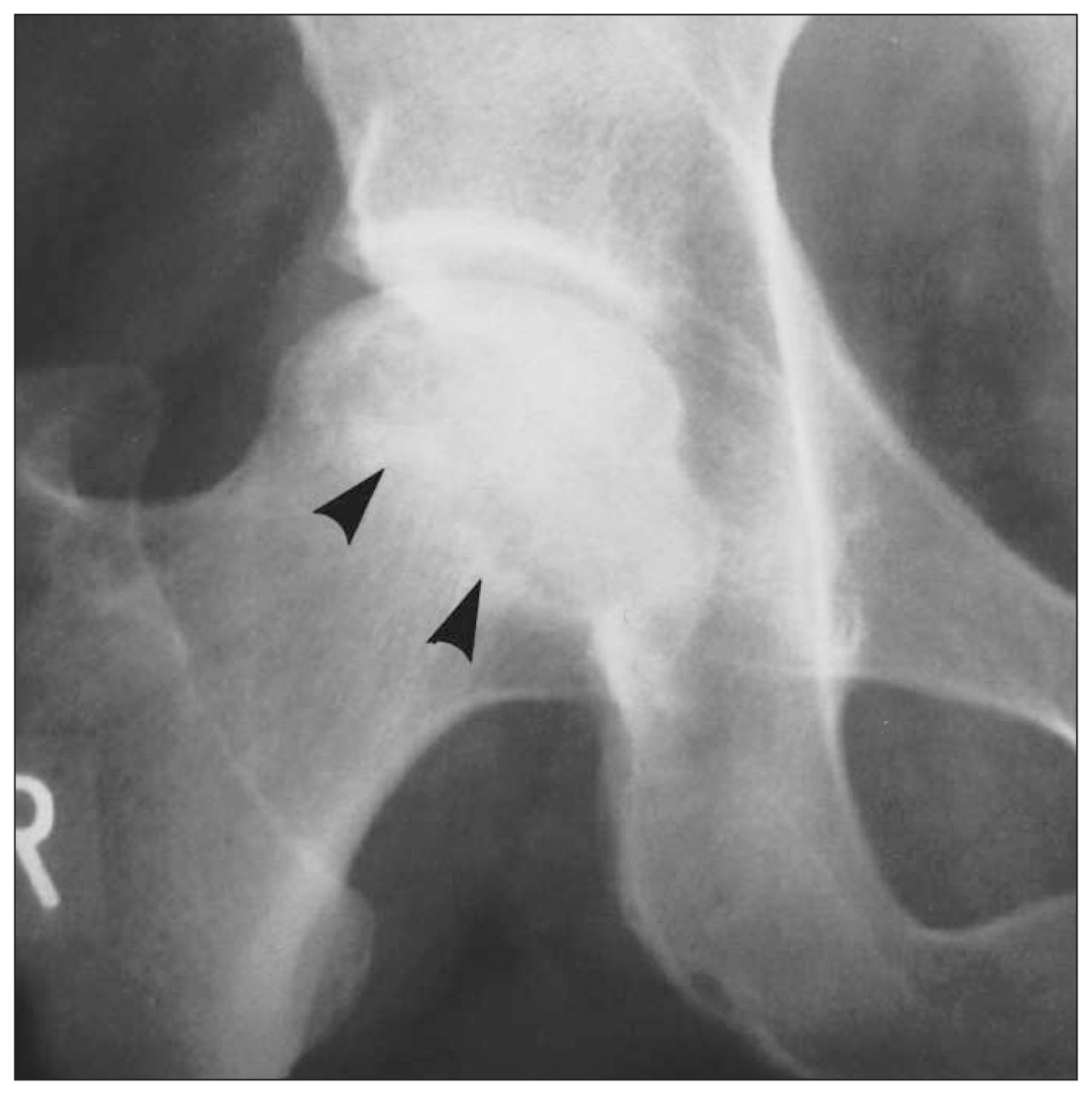
Plain radiograph of the right hip shows a large serpiginous sclerotic area in the right femoral head due to avascular necrosis. Note the distinct sclerotic margin of the lesion in the femoral head (arrowheads).
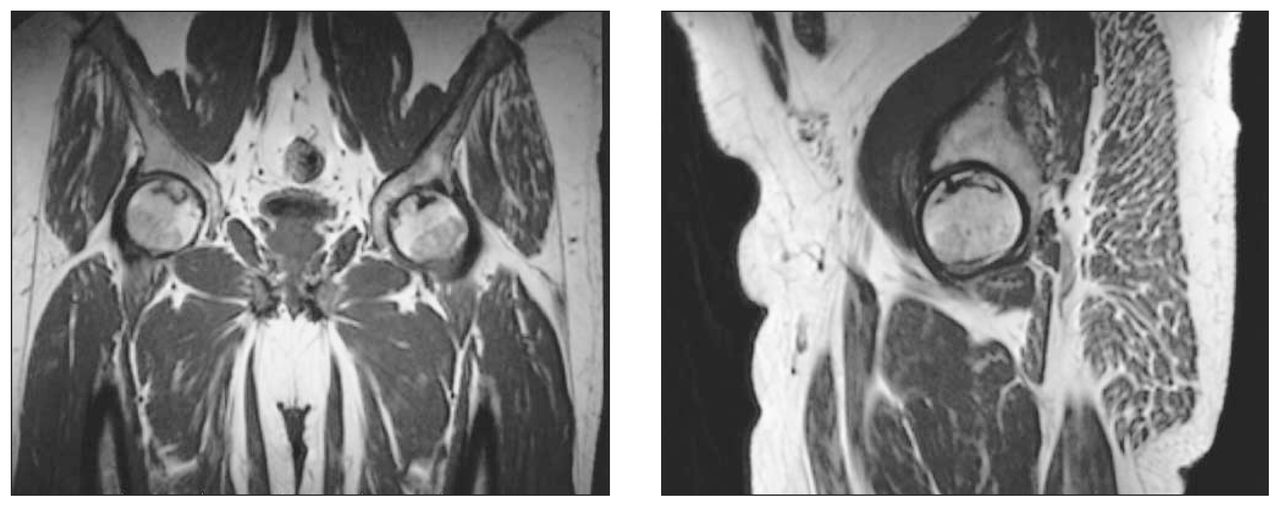
Bilateral avascular necrosis (AVN). A coronal T1-weighted magnetic resonance image of both hips (left) and sagittal T1-weighted image of the right hip (right) shows low-signal-intensity serpiginous lines in the femoral head due to AVN.
Patients 5 and 6 were found to have recurrent TOH, with the second joint affected 5 months and 3 months, respectively, after resolution of symptoms in the first joint. Both patients described symptoms identical to those experienced with the first affected hip; neither radiography nor bone scanning was done. In both cases the diagnosis was established from the MRI findings.
A previous study found that 23 of the 56 patients had recurrent TOH, 9 in the same joint. The higher proportion of recurrences in that study was attributed to a longer period of follow-up (median 73 mo).3 None of our patients has had a local recurrence.
Conclusions
TOH should always be considered in the differential diagnosis of acute hip pain in young men. Symptoms of TOH are sudden in onset and may be severe but resolve over time with reduced weight bearing. The range of movement generally is preserved except for extremes of rotation. In contrast, AVN presents insidiously with progressive pain and marked reduction in the range of movement, especially internal rotation. AVN merits early surgical intervention, and limited weight bearing does little to alleviate the symptoms or the poor natural history of the condition. Radiographs show diffuse osteopenia of the femoral head and neck in TOH but a localized area of sclerosis in AVN, whereas bone scanning shows homogeneously increased uptake in the femoral head and neck in cases of TOH and a localized area of decreased uptake in AVN. MRI shows a diffuse edema pattern common to both entities, but the absence of focal defects and subchondral changes is highly suggestive of TOH. Both physicians and patients should be aware of the possibility of a recurrence of this condition in another joint or in the same joint. Early differentiation of TOH from AVN will avoid unnecessary surgical intervention and ensure appropriate treatment.
Footnotes
Competing interests: None declared.
- Accepted September 23, 2002.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.