


Abstract
Objective: To provide an overview of atlanto-occipital dislocation and associated occipital condyle fractures so as to alert physicians to this rare injury and potentially improve patient outcome. The pertinent anatomy, mechanism of injury, clinical and radiologic evaluation and the management of these rare injuries are discussed in an attempt to alert physicians to this type of injury and to improve outcome.
Data sources: The data were obtained from a MEDLINE search of the English literature from 1966 to 1999 and the experience of 4 spine surgeons at a quaternary care acute spinal cord injury unit.
Study selection: Detailed anatomic and epidemiologically sound radiology studies were identified and analyzed. Only small retrospective studies or case series were available in the literature.
Data extraction: Valid anatomic, biomechanical and radiologic evaluation was extracted from studies. Clinical data came from limited studies and expert opinion.
Data synthesis: Early diagnosis is essential and is facilitated by a detailed clinical examination and strict adherence to an imaging algorithm that includes CT and MRI scanning. When the dislocation is identified, timely gentle reduction and prompt stabilization throuigh nonoperative or operative means is found to optimize patient outcome.
Conclusions: Atlanto-occipital dislocation should be suspected in any patient involved in a high speed motor vehicle or pedestrian collision. Once suspected, proper imaging and appropriate management of these once fatal injuries can improve survival and neurologic outcome.
Traumatic injuries to the occipito–cervical junction have the reputation of being rare and usually fatal. However, these injuries are being diagnosed and treated more frequently, with satisfactory neurologic and functional outcomes. Therefore, early diagnosis of occipitocervical dissociation has become increasingly important. As improved techniques of resuscitation and immobilization at the injury scene result in patients presenting to the emergency physician or surgeon with intact or incomplete neurologic status, failing to make a timely diagnosis may result in catastrophic morbidity and mortality.
Despite the complex functional anatomy between the occiput and the C1 vertebra, there are 2 general injury patterns that occur in this area, atlanto-occipital dislocations (AODs) and occipital condyle fractures. The most severe injury is an AOD. Occipital condyle fractures, on the other hand, appear less serious but can be found in association with severe injuries of the atlanto-occipital complex. 1–4 In this review, we will discuss the mechanism, clinical features, diagnostic imaging and management of these rare occipitocervical injuries.
Atlanto-occipital dislocation
Historically AOD was described in reports of autopsy findings, but improved prehospital and emergency room assessment and care have made AOD an emerging clinical entity. Early autopsy studies reported a 6% to 8% incidence of AOD in trauma fatalities. More recently, autopsy studies and clinical case reports have shown that either this incidence has increased or AOD is more diligently sought. AOD is now estimated to cause 8% to 35% of motor vehicle fatalities and almost 10% of fatal cervical spine injuries.1,2,4–6 The cause of death in most postmortem studies is acute neurogenic shock with neurologic respiratory dysfunction. Many injuries involve pontomedullary brain stem and mid-brain laceration.4
With improved resuscitation, immobilization and imaging techniques as well as increased awareness, there are now over 100 reported survivors in the literature, with approximately 20% being neurologically normal, 10% having cranial nerve deficits, 34% hemiparesis or hemiplegia and 38% high quadriplegia or quadraparesis. Surprisingly, only 24% of patients with AOD had clinical evidence of a closed head injury.7 Other injuries associated with AOD include major facial trauma, mandible fractures, infant airbag injuries and high-energy chest trauma.4,8 Injuries characteristically involve a high-energy mechanism, commonly motor vehicle or motor vehicle pedestrian crashes.6
One of the most significant findings in recent clinical case studies is that the diagnosis of AOD is often delayed or not made in patients who present neurologically intact or have a variety of incomplete neurologic syndromes; this, despite a history including several risk factors. Patients who present with normal neurologic status or an incomplete neurologic injury are at risk for neurologic deterioration, reported to occur in 36% of patients with AOD. The cause is inadequate immobilization of the cervical spine in the course of further diagnostic or therapeutic procedures.7 This preventable morbidity, and the frequent mortality that accompanies it, demands a high level of diagnostic vigilance, particularly because of the increasing prevalence of this injury pattern. The history and physical examination are often limited. Therefore, fastidious attention to detail and a high level of suspicion will enhance the pretest likelihood of identifying this injury and thus dramatically improve the sensitivity of imaging modalities chosen.
Osseous anatomy
The foramen magnum is a large opening in the occipital bone at the base of the skull through which the spinal cord passes. The anterior rim of the foramen magnum is called the basion, and the posterior rim is called the opisthion. Two occipital condyles are situated on the inferior surface of the occipital bone along the anterior lateral edge of the foramen magnum.
The first cervical vertebra supports “the globe of the head” and thus is called the atlas. The atlas is a ring of bone with an anterior and posterior arch and 2 large lateral masses. The concave superior surface of the lateral masses articulates with the occipital condyles, allowing the head to flex and extend. The inferior aspect of the lateral masses is concave and oval. It articulates with the flat convex superior facet of C2, which allows rotation of C1 on C2. The atlas has no vertebral body or spinous process. Functionally, it acts like a bony meniscus between the occiput and C2.
The axis, or C2, is a more conventional vertebra, having a body, lamina and spinous process. It has a superior bony projection from the body, called the odontoid process or dens. The axis pivots or rotates around the odontoid process. The articular processes of the axis are in different planes. The convex superior facets are anterior along the odontoid, allowing rotation. The inferior facets of the axis are posterior and obliquely oriented, similar to the lower cervical facet joints.
Ligamentous anatomy
The morphologic characteristics of the craniocervical articulations accounts for the wide range in neck motion. The internal cranial cervical ligaments include the tectorial membranes, the transverse ligaments, and the alar and apical ligaments. The internal cranial cervical ligaments provide significant biomechanical stability. 9,10 The tectorial membrane and the transverse ligament are located posterior to the dens, limiting anterior atlantoaxial translation. The tectorial membrane is the cranial continuation of the posterior longitudinal ligament. It is a thin, flat ligament that attaches to the foramen magnum anteriorly, and acts to limit extension of the occiput on the axis. Conversely, flexion is limited by impingement of the anterior arch of the atlas on the basion. The transverse ligament attaches to the lateral masses of the atlas medially. The alar ligaments run obliquely, from the tip of the dens to the inner aspect of the occipital condyles. These 2 strong bands limit lateral flexion and rotation. On lateral flexion, the contralateral alar ligament tightens, limiting flexion. With moderate cervical rotation, the ipsilateral alar ligament tightens initially, then shortens and winds around the dens on extreme rotation, allowing the contralateral ligament to tighten and limit further rotation. The tectorial membrane and alar ligament also restrict distraction of the occiput on C1 or C1 on C2. The apical ligament is a vestigial structure located between the tip of the dens and the anterior midpoint of the foramen magnum.
The external cranial cervical ligaments include the ligamentum nuchae, ligamentous flavum, and the anterior and posterior atlanto-occipital membranes, as well as the atlantoaxial membrane. They have little effect on stability.
Neurologic anatomy
Incomplete neurologic syndromes may result from trauma to the medulla, upper spinal cord, cranial nerves and upper cervical nerve roots. The transition from lower brain stem to spinal cord results in a spectrum of neurologic injuries, often involving both structures due to a combination of direct mechanical compression, contusion, laceration, and traction or impaired blood supply, or both. Despite a favourable cord:canal ratio in this region, severe instability predisposes these patients to neurologic injury. Vital centres in the medulla responsible for controlling circulation and respiration may account for the high percentage of fatal injuries. Injury to the brain stem may result in decerebrate posturing. Patients who receive aggressive resuscitation at the injury scene with intubation and ventilation may survive a brain-stem injury.
Vertebrobasilar insufficiency or cerebral or cerebellar infarcts may contribute to the neurologic deficit.11 The carotid, vertebral and anterior spinal arteries are all at risk and can be solely responsible or contribute to many of the neurologic sequelae that occur with this injury. Intimal tears, dissections, thrombosis and subsequent emboli, or complete disruption can occur. A unilateral vertebral injury may cause a clinical syndrome of cerebellar dysmetria or ataxia, ipsilateral cranial nerve V, IX, X and XI deficit, contralateral loss of pain and temperature, and ipsilateral Horner’s syndrome (Wallenberg’s syndrome).
Traumatic spinal cord injury can result in either complete or incomplete cord lesions. One of the more unique incomplete neurologic injury patterns is that of Bell’s cruciate paralysis. Cruciate paralysis is characterized by midline dysfunction of the cephalad portion of the pyramidal decussation. This results in paralysis of the upper extremity with minimal or no lower extremity involvement. The upper extremity motor fibres decussate in a more cephalad and medial position, whereas lower extremity motor fibres decussate in the medulla in a more caudal and lateral position.
Dysfunction of cranial nerves V through XII has also been reported with injuries at the craniovertebral junction. The nucleus of cranial nerve V extends distally in the spinal cord to the level of the C2 vertebra and can be injured along its course. Other cranial nerves course through susceptible foramen, such as the hypoglossal (XII) nerve, which passes through a canal in the occipital condyle where it may be injured by fractures of the base of the skull or condyle. Cranial nerves IX, X and XI are commonly injured, possibly due to their course through the jugular foramen where they may be tethered. The upper cervical nerve roots must be carefully assessed as they can be stretched or avulsed, and their dysfunction may be misinterpreted as a brachial plexus injury.
Mechanism of injury
Occipitocervical instability is caused by high-energy deceleration forces that must overcome the immense dynamic stability provided by the muscular and ligamentous stabilizers of the region. There is a spectrum of injury that includes undisplaced, subluxated and dislocated atlanto-occipital joints. The dislocation or subluxation is usually multi-directional; therefore, no one consistent mechanism exists. Distraction with hyperextension–flexion appears to be the most likely force, often in combination with rotation.2,4,8,12 If the examiner is able to determine the mechanism of injury from an assessment of the history, physical examination and imaging studies, this may guide treatment and facilitate avoidance of inappropriate interventions (i.e., traction).
Imaging
Imaging studies play a pivotal role in the diagnosis and appropriate management of patients with AOD. Despite numerous radiographic criteria and the advent of sophisticated imaging studies such as magnetic resonance imaging (MRI), it remains essential for the clinician to have a clear understanding of the unique bony and ligamentous anatomy of this region to effectively diagnose and manage these patients. Although AOD may be overtly obvious on plain films with severe dislocation, these patients usually die; in survivors, the radiographic diagnosis is often more subtle.
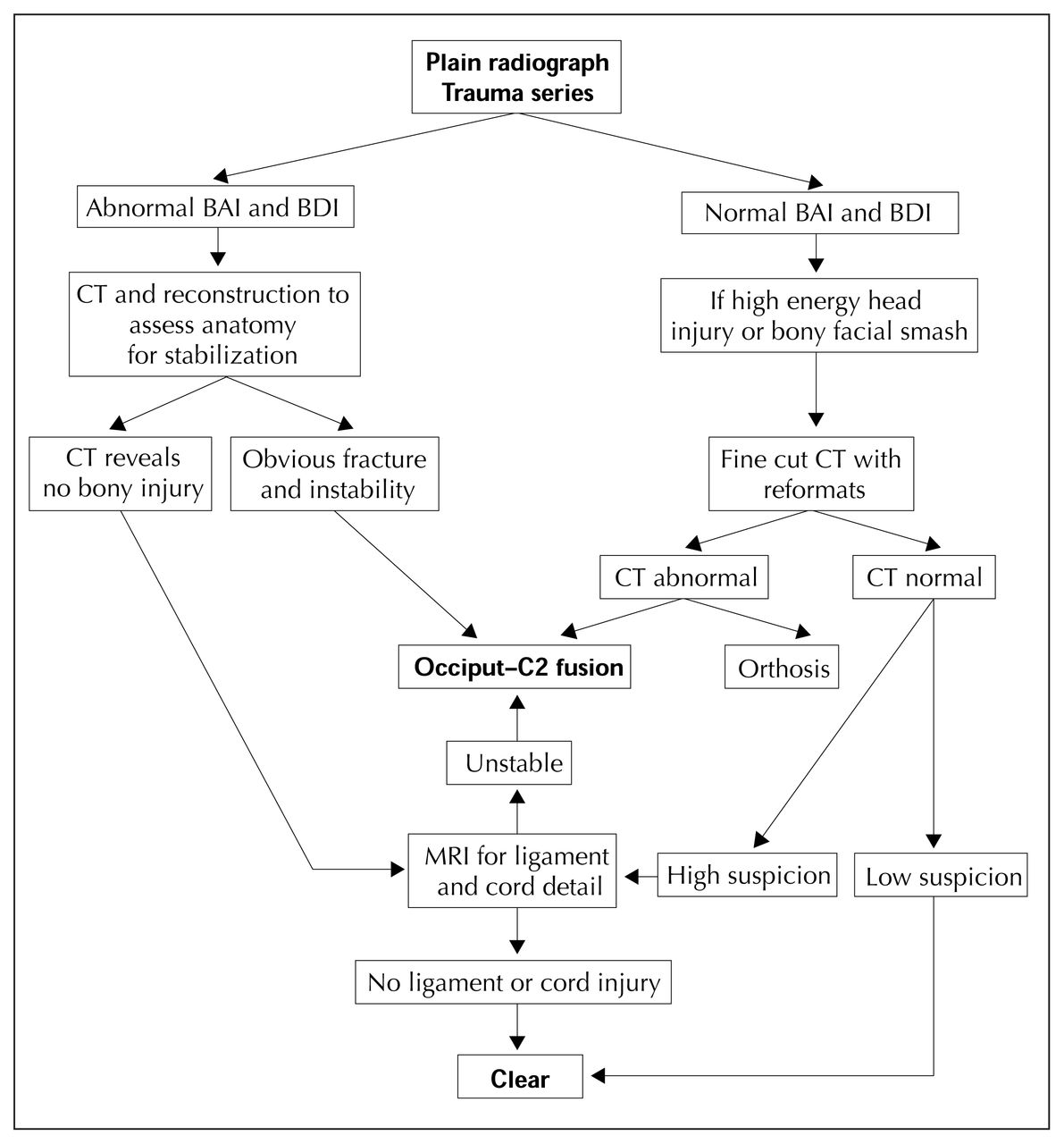
Imaging studies in survivors are often difficult to obtain due to associated injuries and unstable respiratory and hemodynamic status. Despite this, clinicians must follow cervical spine precautions and carefully proceed using an imaging algorithm (Fig. 1) in order to expeditiously identify an occipitocervical spine injury when it is present.

Imaging algorithm to be followed when taking cervical spine precautions in the presence of a possible atlanto-occipital fracture. AP = anteroposterior, BAI = basion–axial interval, BDI = basion-dental interval.
Plain radiographs
Standard anteroposterior, lateral and open-mouth odontoid views are the routine screening radiographs. Careful scrutiny for upper cervical soft-tissue swelling, bone and motion segment relationships will often lead to a preliminary diagnosis. Paravertebral soft-tissue swelling is an important sign but not highly sensitive. More dramatic findings such as free air in the retropharyngeal space, indicating a posterior pharyngeal wall or tracheal disruption would enhance the likelihood of AOD.1,2,13,14 The assessment of bony relationships begins with the occipitoatlantal joints, both on the lateral and open-mouth odontoid films. The general orientation of the basion (the anterior margin of the foramen magnum at the inferior tip of the clivus) with the odontoid process and the relationship of the opisthion (posterior margin of the foramen magnum) to the spinal laminar line provide general alignment guidelines. More specific radiographic criteria have included Powers’ ratio, the X-line, Wackenheim’s clival line and the Wholey method. Because of the variable anatomy, inconsistencies in imaging quality and intrinsic short-comings these parameters are neither reliable nor valid and therefore are not recommended.15,16
The Harris method of detecting AOD derives from a radiographic analysis of 400 adults wherein the basion-axial interval (BAI) and basion-dental interval (BDI) were both determined to be less than 12 mm in normal adults.15 This method is independent of x-ray technique, rotation, tilt, flexion and extension, and appears valid and reliable for determining both normal and abnormal relationships of the atlanto-occipital junction (Fig. 2). Although it has not undergone thorough epidemiologic scrutiny for diagnostic tests, it is easy to remember and currently the best radiographic criterion available. The BDI, measured from the tip of the dens to the basion, should be less than 12 mm and the BAI, measured from the basion to a vertical extension of the posterior cortex of the axis (posterior axis line), should be between 0 and 12 mm. A large value for the BAI suggests anterior displacement (Fig. 3) and a negative value raises the possibility of posterior displacement.

Plain radiograph and schematic diagram demonstrating the relationship between the tip of the dens and the basion (BDI) and the posterior axis line and the basion (BAI), with normal for both being less than 12 mm.

Plain radiograph (top) and sagittal reformat of a CT scan (bottom) showing anterior occipital cervical dislocation with distraction. Both BDI and BAI are greater than 12 mm.
Computed tomography
For many years CT has remained the standard radiologic technique for fractures and dislocations in the craniocervical region. CT with 1.5-mm cuts and reformatting in both the coronal and sagittal planes provides detailed visualization of the bony relationships and congruency of the atlanto-occipital joints.17 A CT scan of the head may demonstrate cranial–cervical junction subarachnoid hemorrhage4,8 or avulsion fractures of the occipital condyles,1,2,18–20 both of which are associated with atlanto-occipital dissociation, and raises the suspicion of severe craniocervical ligamentous injury (Fig. 4). CT with intravenous contrast can also aid in the diagnosis of vascular injuries, particularly the highly susceptible vertebral arteries.21 The limitation of CT in its ability to diagnose ligamentous injuries has been overcome by the detailed soft-tissue imaging available with MRI.

A coronal reformat of a CT scan showing a right occipital condyle fracture in an occipital cervical distraction injury.
Magnetic resonance imaging
MRI is emerging as a valuable adjunct in the diagnosis of atlanto-occipital trauma. MRI is unsurpassed in evaluating ligamentous and neural structures. New sequencing techniques have allowed better visualization of bone, vascular structures and acute hemorrhage. These numerous advantages, along with the need to obtain a timely diagnosis, strongly support MRI as the standard for the evaluation of trauma to the occipito-cervical region.
Specifically, T1-weighted images demonstrate high signal in fat that normally surrounds the odontoid apex and anterior foramen magnum. 22,23 Intermediate to low signal in this region may suggest hemorrhage or edema, indicating possible disruption of neighbouring tectoral, anterior longitudinal, atlanto-occipital membrane and alar ligaments.24 Edema around joint capsules can also be visualized.24 Imaging of the individual ligaments can be accomplished with specific new sequences and image planes; however, the different signal intensities and homogeneity of normal ligaments with standard sequences limits interpretation in some cases.23
T2-weighted images or varied sequences can demonstrate signal change within the spinal cord and brain stem. Measurement of the cervicomedullary angle (normal 135°–175°) can be performed accurately. When this is abnormal (<135°) it has been correlated with neurologic dysfunction.22 Vascular abnormalities and acute hemorrhage, particularly venous bleeding, can also be seen.24 Despite the MRI’s impressive capabilities, it remains very dependent on software, hardware and the operator. Similarly, more work must be done on correlating pathoanatomy with signal characteristics before optimal levels of sensitivity and specificity are obtained. For the present, MRI is an integral part of the imaging armamentarium and is extremely helpful in better defining suspected injuries of the craniovertebral junction.
Classification and management principles
As with all traumatic spinal disorders 3 fundamental issues are considered:; patient factors, stability of the spinal column, and the presence and severity of neurologic injury. The rarity of AOD prevents any clinical trials from effectively evaluating the classification and treatment. Most patients who survive this injury require appropriate assessment and treatment with timely rigid stabilization to prevent neurologic deterioration and to facilitate nursing care. Patients with significant neurologic impairment may benefit from stabilization from occiput to C4 or C5 to provide stability to the head and neck and improve seating in a wheelchair.
Stability is often difficult to assess due to the potential for neurologic injury if any provocative tests (i.e., traction test, flexion–extension views) are used. Therefore, reliance is placed on clinical examination and static imaging studies. A spectrum of displacement occurs with atlanto-occipital dissociation. For example, a high-energy injury mechanism combined with severe neurologic injury, joint subluxation and signal change within the ligament complexes suggests instability. This is especially true if the alar ligaments and tectoral membrane, 2 of the stronger stabilizing structures, are damaged.25,26 Mid-substance tears of these ligaments may be seen on MRI, and avulsion of the alar ligament from the occipital condyle may be inferred from CT images. Pure dislocation leaves little doubt as to a severe capsular ligamentous disruption and grossly unstable injury. When there are associated injuries to C1 or C2, the risk of instability increases.
Neurologic status is determined from careful clinical evaluation and indirectly from interpretation of MRI spinal cord imaging.
Treatment
AOD patients are often multi-traumatized and frequently suffer concomitant neurologic injury. Strict adherence to advanced trauma and life support (ATLS) principles and the treatment of life-threatening injuries is always a priority. Traction, if applied early without sufficient appreciation of the pattern of instability, may lead to further displacement and iatrogenic neurologic injury or worsening.12,27 Sandbags and a hard collar, on the other hand, are less likely to lead to further instability and will provide some splinting as further diagnostic testing is performed. Once AOD is diagnosed, the initial treatment is directed at safely achieving a reduction of the subluxed or dislocated elements and maintaining alignment in a reduced position. Minimal increments of controlled traction may be necessary to achieve a safe closed reduction; however, just as frequently axial compression is required to reduce distracted or translated vertebral segments. 12 These manoeuvres must be performed with careful monitoring of vital signs and neurologic status, fluoroscopic imaging and minimal application of force. Reduction, when there is neurologic deficit, should be performed as soon as possible as this is often the most expeditious technique of indirectly decompressing the neurologic structures.
Definitive stabilization and maintenance of alignment may be achieved through the use of orthotics or surgical stabilization. Patient factors such as the presence of associated injuries, size and weight, nursing concerns, functional expectations, and others must be considered. Early rigid internal fixation is recommended in the multitraumatized patient as it has been shown to improve outcome by facilitating mobilization. The patient with a mandible fracture will not tolerate a brace, which rests on the mandible, and thus may be better treated with surgical stabilization. If subluxation is minimal or absent, the injury may be relatively stable and can be treated with an orthosis and careful monitoring. Only the halo-thoracic vest affords stability to this region. The Minerva and other types of cervical orthosis are not recommended for stabilization of the occipitocervical region.
The presence of a significant neurologic injury is highly suggestive of an underlying unstable bony or ligamentous injury. The neurologic insult may occur secondary to direct spinal cord compression, resulting from subluxation or dislocation with or without fractures. MRI, initially obtained to evaluate the severity and location of the neurologic insult may provide evidence of ligament injury, which may suggest mechanical instability. Ligament injuries do not heal well in the spine and when the predominant injury is ligamentous without significant bony fracturing, rigid surgical stabilization is recommended to prevent further neurologic injury and facilitate rehabilitation.28
Successful results have been reported when the surgical goal has been to obtain an occiput to C2 fusion. 28 This has been achieved using a spectrum of techniques including the use of onlay autogenous bone grafts, various interspinous and occipital wires and graft constructs, internal fixation with sublaminar wires fixed to pre-bent rods or pins, and screw-plate constructs (Fig. 5). The specific pathoanatomy of the patient, resource availability, surgeon preference and surgeon experience all play a role in the chosen technique. Depending on the rigidity of the internal stabilization and the functional demands of the patient, the surgeon may supplement the surgical stabilization with varying degrees of external immobilization including traction, halo-thoracic vest or a removable orthosis. Fusion across the occiput to C2 complex significantly limits cervical rotation and flexion–extension. In the patient with a high lesion spinal cord injury, this loss of motion may improve head and neck positioning in the sitting position. As with any fusion, fastidious attention to proper grafting technique and the use of autogenous bone will optimize the radiographic success rate of the fusion. Our preferred technique provides rigid internal fixation and limits the need for external bracing (Fig. 6).

A 40-year-old patient who had a distraction-type occipitocervical injury demonstrated radiographically in the BDI (arrowheads). This patient required occiput to C2 stabilization.

Occiput–cervical fusion in a high tetraplegic patient after atlanto-occipital dislocation, requiring occiput to C3 stabilization.
Outcome
Once the fusion is solid, biomechanical studies suggest the patient’s sagittal range of motion will be reduced by 23°, rotation by 50° and lateral flexion by 8°.29 If the patient is neurologically intact, the outcome would be similar to that for other conditions requiring fusion across the occipito–cervical junction. With a neurologic deficit, the prognosis is more difficult to predict. Patients having a complete high lesion spinal cord injury will be dependent on ventilatory support but may live in the community with portable home ventilators. For incomplete lesions, the patient’s progress and outcome may be quite remarkable, thus the importance of a careful neurologic examination, particularly the perianal examination, at the time of the patient’s initial presentation.
In summary, atlanto-occipital dissociations are rare but must always be suspected in the multitraumatized patient with a compatible mechanism of injury and head or facial trauma. Strict maintenance of cervical spine precautions and adherence to an imaging algorithm is imperative. In the presence of an occipitocervical injury the goal is to preserve or improve neurologic status by timely reduction and then to provide stabilization through nonoperative or operative means, depending on the degree of instability, the severity of neurologic injury and the patient’s general status.
Occipital condyle fractures
Many of the anatomic and biomechanical concepts already discussed apply to occipital condyle fractures. These injuries are rarely diagnosed, most likely due to a low incidence and a tendency of these injuries to go unrecognized as the majority have a relatively benign course. The true incidence is unknown, but in a study of 21 patients with blunt craniocervical trauma, 19% had occipital condyle fractures.30 There is a strong association with contiguous and noncontiguous spinal fractures, especially of the axis and atlas.
Occipital condyle fractures are usually unilateral and often isolated. They can be associated with head injury and facial fractures. Unlike AODs, these fractures can occur with both low- and high-energy trauma. The most common mechanism of injury is an axial load with or without a shear, rotation or lateral flexion force.31 Depending on the mechanism and force of the injury, the occipital condyle fracture can occur in isolation or as part of a more complex atlanto-occipital dissociation.1,2
Clinical features
Patients with occipital condyle fractures present with a spectrum of symptoms. An isolated low-energy fracture may present with suboccipital neck pain, decreased range of motion or spasmodic torticollis, whereas a high-force event causing multiple trauma presents similarly to AODs.32,33 Careful attention must be paid to spinal cord, cranial nerve and upper cervical nerve root function. Vascular injuries resulting in vertebrobasilar symptoms must also be suspected.33
Imaging
Initial screening lateral and open-mouth odontoid radiographs will often miss occipital condyle fractures because of the overlying complex facial bone anatomy. Retropharyngeal or pre-vertebral soft-tissue swelling and occipital condyle joint asymmetry may be seen. The study of choice for condyle fractures is fine cut (1 mm) CT with coronal and sagittal reformatting, which provides excellent bone and joint detail.33 Small fragments in the region of the condyle suggest ligamentous avulsion and potential instability. Lateral subluxation of the occiput–C1 joint less than 11 mm is not associated with instability.33 In the setting of closed head injury or multitraumatized patients in whom the history and physical examination are limited, the routine CT of the head should include bone window cuts through the occipital C1 complex. The findings on a standard head CT are not sufficiently detailed to classify these injuries and determine appropriate treatment, so the fine-cut CT protocol should be used if a fracture is suspected. If clinical suspicion is high, MRI may be indicated to assess the integrity of the ligamentous and capsular anatomy.
Although the occipitocervical joint is a mobile synovial joint that transmits significant load through a range of motion, symptoms of posttraumatic osteoarthritis have not been reported. These symptoms, however, may be camouflaged by the commonly associated head injury, contiguous cervical spine fracture or may be attributed to cervical soft-tissue strain.
Treatment
If an occipital condyle fracture is associated with AOD, treatment of the AOD should take precedence to ensure stability of the atlanto-occipital joint as already mentioned. With isolated occipital condyle fractures good results have been achieved with external immobilization with orthotics or a halo-thoracic vest.34
- Accepted October 2, 2000.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.