


Abstract
Background: Obesity is associated with increased mortality. Bariatric surgery is becoming an important treatment modality for obesity, with an associated reduction in mortality. There are few data available on the incidence and cause of death in referred patients while they are waiting for bariatric surgery.
Methods: We retrospectively examined all cases of death in patients who were referred for bariatric surgery assessment but who had not yet undergone bariatric surgery at a tertiary care centre in Halifax, Nova Scotia. The wait list comprised patients referred for surgery between March 2008 and May 2013. All cases of death were reviewed to determine age, sex, time of referral, time spent on the wait list, cause of death, comorbidities and body mass index (BMI).
Results: Of the 1399 patients referred, 22 (1.57%) died before receiving surgery. The mean age of these patients was 62.7 (range of 32–70) years. The average time from referral to death was 21.6 months, and the average BMI was 51.5. The most frequent cause of death was cancer, followed by cardiac and infectious causes.
Conclusion: This study provides useful information about mortality and causes of death among patients awaiting bariatric surgery at our centre. Our results will help guide the development of a judicious system for triage in light of long wait times.
The obesity epidemic is upon us. Approximately two-thirds of North Americans have a body mass index (BMI) above the reference range of 18.5–24.9.1 In a recent analysis of weight trends in Canadians, there was a 200% increase in obesity (BMI ≥ 30) from 1985 to 2011. The rate of change was greater for each successively higher BMI class. In 2011, 18.3% of Canadians were obese; this percentage is expected to increase to 21% by 2019.2 In Atlantic Canada, the problem is worse, as shown by an obesity rate that is significantly higher than the national average.3 The medical costs of people with a BMI of 30 or greater have been shown to be 30% greater than those of people with a BMI under 25.4 In 2006, the direct cost of obesity on the Canadian health care system was approximately $6 billion, which corresponds to 4.1% of total health expenditures.5 Obesity is also strongly associated with increased risk of death across all age groups, races and sexes.6 In Canada, 9.3% of deaths were attributable to overweight and obesity in 2000.7 In a collaborative analysis of 57 prospective studies, each 5 kg/m2 increase in BMI was associated with a 30% higher mortality. A BMI of 30–35 was associated with a reduction in median survival of 2–4 years, and this reduction was 8–10 years for a BMI of 40–45.8 While pharmacologic and lifestyle measures produce modest weight loss, bariatric surgery has been shown to produce a substantial and sustained weight loss as well as improvement or resolution of obesity-related comorbidities.9 In the Swedish Obese Subjects study, a prospective controlled trial evaluating bariatric surgery in 2010 obese participants compared to usual care in 2037 matched obese controls, the primary end point, mortality, was reduced by 29% in those who received surgery.10
The current indications for bariatric surgery are based on the National Institutes of Health (NIH) consensus conference in 1991.11 The requirements include a BMI of 40 or greater or a BMI or 35 or greater combined with a clinically important comorbidity, such as diabetes, hypertension or dyslipidemia. While there is no formal list of clinically important comorbid conditions, it is sufficient that the patient’s quality of life and overall health is affected. Over time, indications for bariatric surgery have become even more inclusive. In February 2011, the U.S. Food and Drug Administration announced that the Lap-Band, an adjustable gastric band, was approved for use in the United States for patients with a BMI of 30 or more who had an associated comorbidity.12 The International Diabetes Federation released a position paper in March of 2011 stating that surgery should be considered for patients with a BMI of 30–35 when diabetes cannot be adequately controlled by an optimal medical regimen.13 With rising obesity rates and loosening eligibility criteria, Canadian provincial health care systems are struggling to handle the surging demand for bariatric surgery.
In 2007, the estimated average Canadian wait time for bariatric surgery was more than 5 years; this estimate was based on 1313 surgeries performed at 12 major Canadian centres.14 It has been estimated that 5.8% of Canadians — approximately 2 million people — may be eligible for bariatric surgery.15 Based on data from the Canadian Health Measures Survey, 1.5 million obese Canadian adults met the eligibility criteria for bariatric surgery in 2007–09. Of those, only 0.1% underwent publicly funded bariatric surgery.16 Accordingly, the number of surgeries being offered in Canada has increased over time, particularly in Quebec and Ontario. Furthermore, a number of private centres offering adjustable gastric banding have been established. In 2009, there were 30 clinics across Canada (18 public and 12 private) and 53 surgeons performing this procedure. It was found that the average wait time for surgery in a private clinic was 1 month and that the average out-of-pocket cost was approximately $16 000.17 It is uncertain at the present time how many patients are using the private clinics in Canada or paying for surgery in the United States or further abroad, where prices may be considerably different.
As might be expected, patients who are eligible for surgery tend to have higher rates of comorbidities and inferior self-rated mental health and quality of life than ineligible patients.16 When surveyed, 86% of patients on a wait list for bariatric surgery reported worsening physical symptoms during the wait, and almost half felt that the waiting affected their quality of life.18 Given that the relative risk of death after bariatric surgery is reduced in as little as 5 years, we may be placing obese individuals at higher risk by delaying surgery.19 The goal of the present study was to determine how many patients were referred for bariatric surgery at our institution and to estimate an approximate wait time for surgery. Also, recognizing the higher disease burden in this population, we aimed to determine the number and cause of any deaths among patients awaiting bariatric surgery.
Methods
As part of a quality assurance effort, we examined patient referrals for bariatric surgery at our tertiary care centre in Halifax, NS, from March 2008 to May 2013. We reviewed the charts of patients who died while waiting for surgery to identify the time of referral for bariatric surgery, the referring physician and his/her specialty, the patient’s age at death, sex, birth date, height, weight, BMI, comorbidities and cause of death. The bariatric surgery eligibility criteria at our centre are based on the NIH consensus conference, and this information was made available to referring physicians through a bariatric surgery referral template. Patients were considered to be on the wait list from the time the referral was received. At a later stage, the surgeon and nurse practitioner further assess the suitability of the patients on the wait list for surgery. The main sources of information were the referral letters, death summaries, death certificates, inpatient progress notes, ambulatory clinic letters and diagnostic test reports. The Department of Vital Statistics provided data on cause of death when this information was not available in the patients’ charts.
Statistical analysis
We used the χ2 test to compare mortality in our cohort to the reported Canadian all-cause mortality.
Results
There were 1399 referrals for evaluation for bariatric surgery between March 2008 and May 2013. Twenty-two deaths were observed in the cohort of patients who were referred. The average age at death was 62.7 (range 32–70) years. Fifty-nine percent of deaths occurred in men. The demographic and clinical characteristics of patients who died are listed in Table 1. The average BMI for the group was 51.5 (range 35.0–64.9). In terms of type of physician generating the referrals, 31% came from endocrinologists, 38% from general practitioners, 23% from other internists and 7.7% from surgeons. The average time from referral to death was 21.6 months.
Patient demographic and clinical characteristics
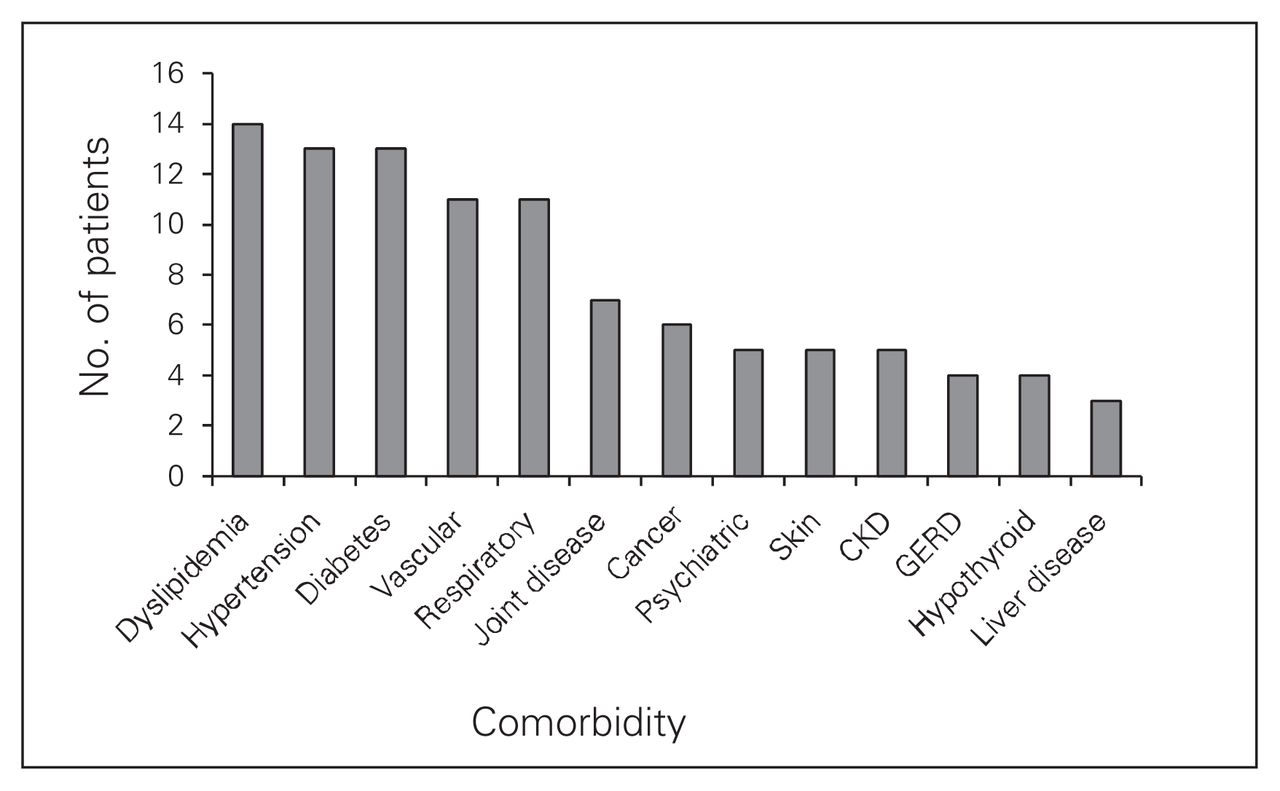
Figure 1 illustrates the type and frequency of patient comorbidities. The average number of comorbidities per patient was 6.9. The less common comorbidities, such as pancreatitis, renal stones and cholelithiasis, occurred in fewer than 3 patients each, and they are not included in Figure 1.
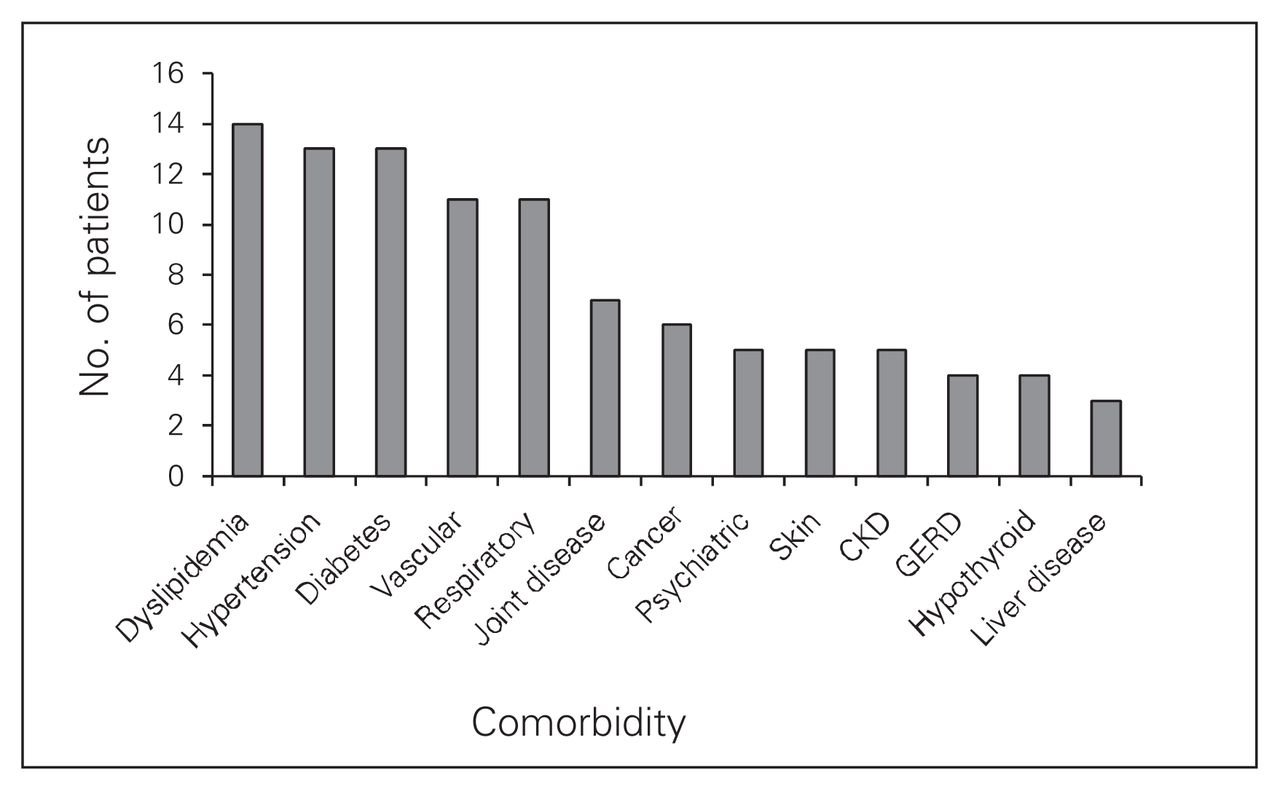
The comorbidities of the 22 deceased patients in our series. Less common comorbidities (n < 3) are not shown. “Vascular” includes coronary artery disease, peripheral vascular disease and stroke. “Respiratory” includes obstructive sleep apnea, asthma and obesity hypoventilation syndrome. CKD = chronic kidney disease; GERD = gastresophageal reflux disease.
Information on cause of death was not available for 5 of 22 patients. Overall mortality in our study was 1.57%, which is a significant 3.21-fold increase (p < 0.001) compared with the all-cause, age-standardized mortality of 0.49% reported for Canadians in 2011.20 Figure 2 demonstrates the cause of death by category. The most common cause of death was cancer, occurring in 5 patients (23%); the subtypes were esophageal, breast, lung, melanoma and cancer of unknown primary (presumed pancreatic). Cardiac-related deaths occurred in 4 patients (18%). Three patients died of infectious causes (14%), including 1 patient who died of methicillin-resistant Staphylococcus aureas (MRSA) pneumonia and sepsis, 1 patient who died of MRSA cellulitis and sepsis, and 1 patient who died of sepsis from an infected hip shortly after a total hip replacement. Two patients died from pancreatitis (9%), 2 from respiratory causes (9%) and 1 from renal disease (5%).
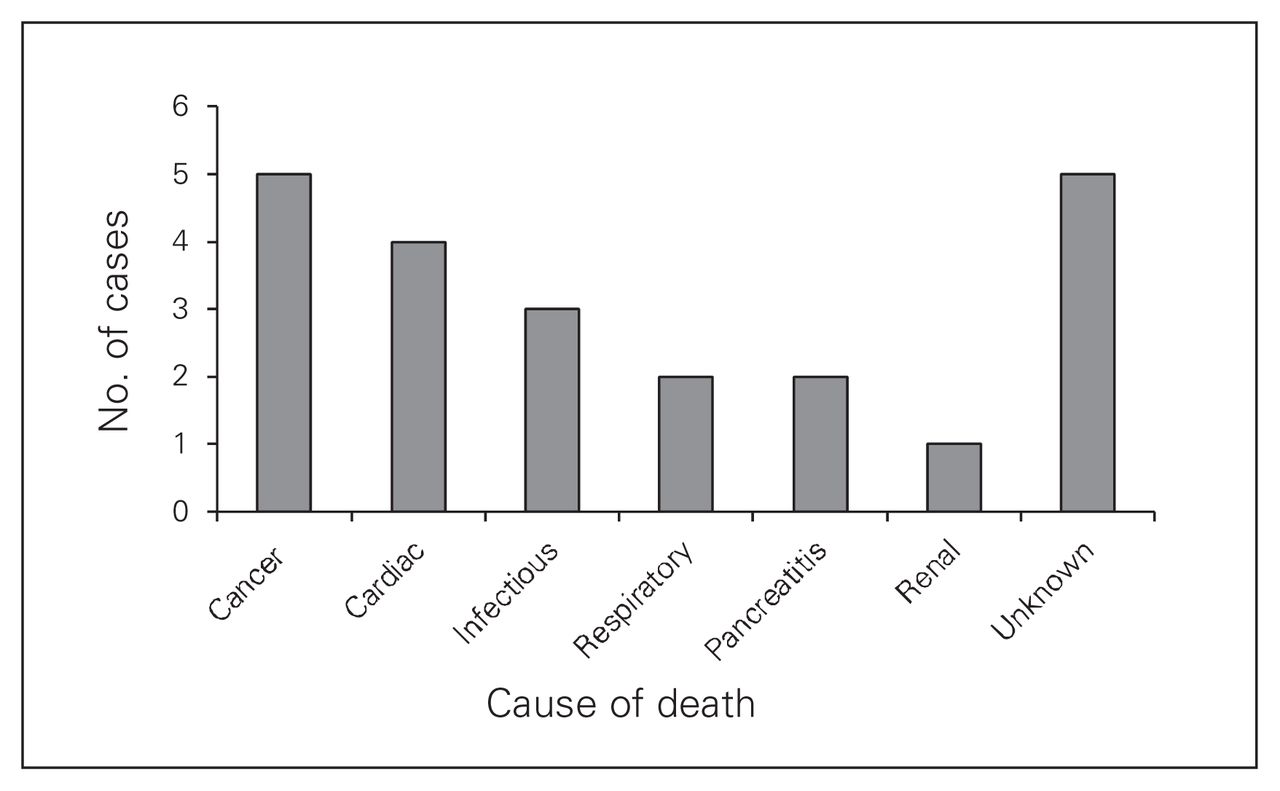
Cause of death among patients in our series. The number of cases for each cause of death category is shown. The cause of death could not be determined in 5 patients.
Discussion
This case series examined the number of deaths that occurred in our cohort of patients referred for bariatric surgery. Of the 1399 referrals received, 22 deaths occurred before the patients received bariatric surgery. This mortality of 1.57% is 3-fold higher than in the age-standardized general population. From this data, we were able to estimate an approximate wait time for surgery from the time of referral. Given the current rate of 80 laparoscopic sleeve gastrectomies performed per year at our centre and 1399 referrals, it would take approximately 17.5 years to handle the current volume, assuming no further referrals are received. Granted that not all patients referred for bariatric surgery are appropriate candidates, this figure is nonetheless well above the national wait time of 5.2 years described in 2007.14
As one might expect, Canadian patients awaiting bariatric surgery describe the experience as stressful, anxiety-provoking and frustrating, with many expressing anger toward the health care system.21 At present, there is no universally accepted and judicious approach to triaging patients for bariatric surgery. In a recent survey of patients awaiting bariatric surgery, most patients felt that those with more functional impairment and greater clinical severity should have a higher priority on the wait list. Most patients also disagreed with out-of-pocket payment for faster access to bariatric surgery.22 The aim of our study was to identify the causes of death in this population to gain a better understanding of who is at highest risk.
A 2009 study by Christou and Efthimiou14 examined the bariatric surgery wait list at another Canadian centre. The patients who died on their wait list were similar to our own cohort in terms of the average age, BMI, sex ratio and number of comorbidities. In our cohort, the 3 primary causes of death were cancer, cardiac death and infection. The cancer-related deaths were from metastatic breast, melanoma, lung, esophageal as well as a cancer of unknown primary that was presumed on autopsy to be pancreatic cancer. According to the chart and referral, none of the cancers was present at the time of enrolment onto the wait list. From a large prospective study involving more than 500 000 adults in the United States, it has been estimated that overweight and obesity account for 14% of all cancer deaths in men and 20% of all cancer deaths in women.6 The Prospective Studies Collaboration found that for each 5 kg/m2 increase in BMI above the reference range there was an associated 10% increase in cancer-related mortality.8 The specific cancer sites with the highest rates were liver, breast, colon, endometrium, kidney and prostate.8 The authors also reported a 39% higher incidence in mortality from ischemic heart disease for each 5 kg/m2 increase in BMI above the reference range. In our study, the infection-related deaths were from sepsis resulting from pneumonia, cellulitis and surgical site infection following hip replacement. Obesity is considered to be a state of chronic inflammation and has been shown to negatively impact host defence and immune function.23 Not only is there a higher risk of skin infections and cellulitis in general, but the risk of surgical site infection is increased up to 5-fold in obese individuals, although this increase may correlate more closely with percent body fat than BMI.24
This study highlights the characteristics of patients who died after referral for bariatric surgery, demonstrating a 3-fold higher mortality than in the general population. Our results allow us to understand the number and types of comorbidities as well as the increased frequency of cancer, cardiac and infectious causes of death in this population. Future studies will be focused on identifying how this cohort of deceased patients compares to the remainder of the referred patients at our centre. Given the limited resources and the trends in obesity, we wish to focus attention on issues of wait list management. Our objectives are to develop an equitable strategy to better triage this vulnerable population for bariatric surgery.
Footnotes
Competing interests: None declared.
Contributors: All authors designed the study and analyzed the data, which J. Lakoff acquired. J. Lakoff wrote the article, which all authors reviewed and approved for publication.
- Accepted June 2, 2014.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.