


Abstract
Background: We sought to determine the efficacy of sutures, human fibrin glue and N-butyl-2-cyanoacrylate for mesh fixation in patients undergoing the plug and mesh procedure for groin hernia.
Methods: A total of 156 patients with 167 inguinal hernias (11 bilateral) underwent a plug and mesh procedure and were randomly assigned to received either sutures (n = 59 hernias), human fibrin glue (n = 52) or N-butyl-2-cyanoacrylate (n = 56) for mesh fixation.
Results: The overall morbidity rate was 38.98% in the suture group, 9.62% in the fibrin glue group and 10.71% in the N-butyl-2-cyanoacrylate group (suture v. fibrin glue, p < 0.001; suture v. N-butyl-2-cyanoacrylate, p < 0.001). There was no significant difference in morbidity between the fibrin glue and N-butyl-2-cyanoacrylate groups. Overall, short-term morbidity was significantly higher in the suture group (27.12%) than in the fibrin glue (9.62%, p = 0.01) or N-butyl-2-cyanoacrylate (8.93%, p = 0.004) groups, but there was no significant difference between the fibrin glue and N-butyl-2-cyanoacrylate groups. There was no significant difference between the groups in terms of mean postoperative stay (32.6 h in the suture group v. 30.8 h in the fibrin glue group v. 32.0 h in the N-butyl-2-cyanoacrylate group) or mean time to return to work (20.4 d in the suture group v. 20.3 d in the fibrin glue group v. 19.8 d in the N-butyl-2-cyanoacrylate group). Overall, long-term morbidity was significantly higher in the suture group (11.86%) than in the fibrin glue (0%, p = 0.001) or N-butyl-2-cyanoacrylate (1.78%, p = 0.03) groups. There was no recurrence in any of the groups. Two cases (3.39%) of chronic groin pain were reported in patients in the suture group. A sensation of extraneous body was reported in 5 (8.47%) patients who received sutures and in 1 (1.78%) patient in the N-butyl-2-cyanoacrylate group; there were no reported cases in the fibrin glue group (suture v. fibrin glue, p = 0.01; suture v. N-butyl-2-cyanoacrylate, p = 0.03; fibrin glue v. N-butyl-2-cyanoacrylate, p = 0.30).
Conclusion: The use of human fibrin glue or N-butyl-2-cyanoacrylate is better tolerated than sutures in tension-free inguinal open repair using the plug and mesh technique in terms of overall immediate results, and there is a better trend in the long-term data.
The incidence of symptomatic inguinal hernias is about 16% in adult men. Groin hernioplasty is the most common operation in general surgery and is one of the top 3 surgical procedures in most Western countries.1,2 The morbidity and recurrence rates have decreased in the last 2 decades because of the introduction of open tension-free hernia surgery with mesh. Nevertheless, the incidence of recurrence in nonspecialized centres is still high,3 and postoperative pain and discomfort are common.4 Some authors have reported an incidence of chronic pain of 10%–30% of among patients who underwent inguinal hernia repair.5,6
Plug and/or mesh procedures for inguinal hernia open repair are minimally invasive, easy to perform and popular. They use standardized techniques (i.e., Trabucco, Rutkow and Robbins, Lichtenstein) with a low recurrence rate and morbidity.4 However, complications associated with sutured mesh fixation following open groin hernia repair, such as chronic irritation and pain, are probably due to tension or nerve compression by the sutures; these complications have prompted surgeons to use atraumatic methods of fixation, such as human fibrin glue and cyanoacrylate.
Fibrin sealant (Tissucol; Baxter Healthcare) is a biodegradable adhesive that combines human-derived fibrinogen and thrombin activated by calcium chloride. It has been available commercially for more than 20 years and has been proven to be effective in numerous clinical applications.7–10 In addition to its hemostatic action, the fibrinogen component gives the product tensile strength and adhesive properties,11 and this component promotes fibroblast proliferation.12 Cyanoacrylate has been used as a surgical tissue adhesive since the 1960s.13 Glubran 2 (GEM Srl) is a new cyanoacrylate surgical glue composed of N-butyl-2-cyano-acrylate and methacryloxysulfolane monomer. The longer radical chain has a lower temperature of polymerization than histoacryil, which results in lower toxicity and fewer inflammatory reactions.14,15 It has been used for many procedures including skin closure of abdominal wounds,16 suture reinforcement,17 arteriovenous embolization,18 endoscopic treatment of bleeding gastroduodenal ulcers and varices,19 occlusion of external biliary fistulas refractory to endoscopic drainage,20 endoscopic closure of pancreatic fistulas21 and fixation of polypropylene mesh in open13,22 and laparoscopic hernia repair.23 However, the use of these glues increases the costs of hernioplasty compared with sutures.
Our aim was to compare the short-term outcomes (pain, local numbness, hematoma, seroma, wound infection, urinary retention), long-term outcomes (chronic pain, sensation of extraneous body, recurrence), operation time and the time to return to work for patients who underwent a plug and mesh procedure for open groin hernia repair with sutures, human fibrin glue or N-butyl-2-cyanoacrylate for mesh fixation.
Methods
Patient selection
From Jan. 1, 2003, to Dec. 31, 2007, we selected 169 patients from those undergoing surgery for groin hernia repair at our academic hospital. Twelve of these patients were lost during follow-up and 1 died in a motor vehicle collision. Routine preoperative anesthesia assessment was performed. We included patients aged 16 years or older with evidence of primary inguinal hernia, those undergoing a plug and mesh procedure during elective surgery by the same surgeon (M.T.), who has experience in inguinal hernia surgery, and those using epidural anesthesia. We excluded patients who received emergency surgery, those with recurrent or giant hernias, those with chronic obstructive pulmonary disease or disorders of hemostasis and coagulation, and those whose surgery used a laparoscopic approach.
Randomization was performed using numbered and sealed envelopes that were opened at the beginning of the operation. If a bilateral hernia was present, the patient was assigned to one group and both hernias received the same treatment. All patients gave written informed consent before inclusion in the study.
Procedure
Antibiotic prophylaxis was given as a single dose of a third-generation cephalosporin. After the surgeon opened the external oblique aponeurosis, the spermatic cord was separated from the posterior wall and dissected; the ilioinguinal, genitofemoral and iliohypogastric nerves were identified when possible and carefully preserved. In cases of bilateral hernia, each one was treated individually; the second operation began when the first was finished in order to time each operation precisely.
All of the operations were performed using a preshaped monofilament knitted polypropylene mesh and plug (mesh PerFix plug; Bard). In some cases, the mesh was shaped to the inguinal canal. The spermatic funiculus was opened and dissected and, for both indirect and direct hernias, a plug was used for occlusion of the internal orifice and a mesh was applied on the transversalis fascia. If a direct hernia sac was present, the transversalis fascia was strengthened with an uninterrupted single layer of 3/0 polypropylene sutures and the mesh was positioned on this layer. For the groups that received either fibrin glue or N-butyl-2-cyanoacrylate, the glue was applied all over the mesh (2 mL fibrin glue or 1 mL N-butyl-2-cyanoacrylate).
Outcomes
Patients were monitored after surgery until hospital discharge. They were evaluated by physical examination on days 3, 7 and 15 and at 1, 3, 6 and 12 months after surgery. We evaluated short-term outcomes (pain, local numbness and hematoma, seroma, wound infection and urinary retention), long-term outcomes (chronic pain, sensation of an extraneous body, recurrence), length of operation and time to return to work. For patients who did not work, we evaluated the return to normal activity (i.e., walking, driving, sports). We defined short-term morbidity as the complications observed within 1 month after surgery and postoperative pain as a postherniorrhaphy pain that required analgesia. We defined chronic pain as pain that persisted for more than 3 months after surgery24 and as pain that caused social disability and limited normal activity (e.g., walking, driving, playing sports, standing more than half an hour, working). At the follow-up physical examinations, we evaluated postherniorrhaphy pain using a questionnaire5 that described the localization, frequency and level (slight, moderate, severe). We also recorded the frequency of use of systemic analgesic therapy.
Statistical analysis
We performed a double-blinded randomized controlled study by calculating the sample size before the trial that would give 80% power at a 2-sided 5% significance level to detect a difference in the recurrence rate of 50%. The results are presented as mean and standard deviation (SD). We used the Student t test to compare the data sets and the χ2 test to assess associations between categorical data. We considered a p value of less than 0.05 to be statistically significant.25,26 We performed calculations using NCSS 2007 and GESS 2006 statistical software (version 07.1.4).
Results
Table 1 presents the side, size, type of the hernia and sex of the patients. In total, we included 156 patients (12 women and 144 men; mean age 58, range 17–85 yr) with 167 hernias (11 bilateral). Bilateral hernia was observed in 11 (7.1%) patients. The patients were randomly assigned to receive either sutures (n = 53 patients with 59 hernias), in which the mesh and plug were fixed with 5–6 interrupted 3/0 polypropylene monofilament sutures, or fibrin glue (n = 49 patients with 52 hernias) or N-butyl-2-cyanoacrylate (n = 54 patients with 56 hernias) for mesh and plug fixation. The mean length of follow-up was 30 (range 14–60) months in the suture group, 29 (range 12–60) months in the fibrin glue group and 30 (range 12–60) months in the N-butyl-2-cyanoacrylate group.
Characteristics of patients who underwent plug and mesh hernia repair with sutures, human fibrin glue or N-butyl-2-cyanoacrylate
The mean duration of surgery was 54.5 (SD 11.44) minutes in the suture group, 56.2 (SD 8.87) minutes in the fibrin glue group and 54.2 (SD 10.40) minutes in the N-butyl-2-cyanoacrylate group. There was no significant difference among the groups for this outcome. No intraoperative complications occurred during surgery in any of the groups. The overall morbidity rate was 38.98% in the suture group, 9.62% in the fibrin glue group and 10.71% in the N-butyl-2-cyanoacrylate group (suture v. fibrin glue, p < 0.001; suture v. N-butyl-2-cyanoacrylate, p < 0.001; fibrin glue v. N-butyl-2-cyanoacrylate, p = 0.85). The short-term complications are summarized in Table 2. The incidences of postoperative pain, local numbness and hematoma were significantly higher in the suture group than in the glue groups. The hematomas healed without drainage or reoperation. None of the patients reported severe postherniorrhaphy pain, and none of the patients required reoperation.
Short-term outcomes among patients who underwent plug and mesh hernia repair with sutures, human fibrin glue or N-butyl-2-cyanoacrylate
The mean length of postoperative stay in hospital was 32.6 (SD 13.39) hours in the suture group, 30.8 (SD 12.96) hours in the fibrin glue group and 32.0 (SD 13.18) hours in the N-butyl-2-cyanoacrylate group (p = 0.70) (Fig. 1).
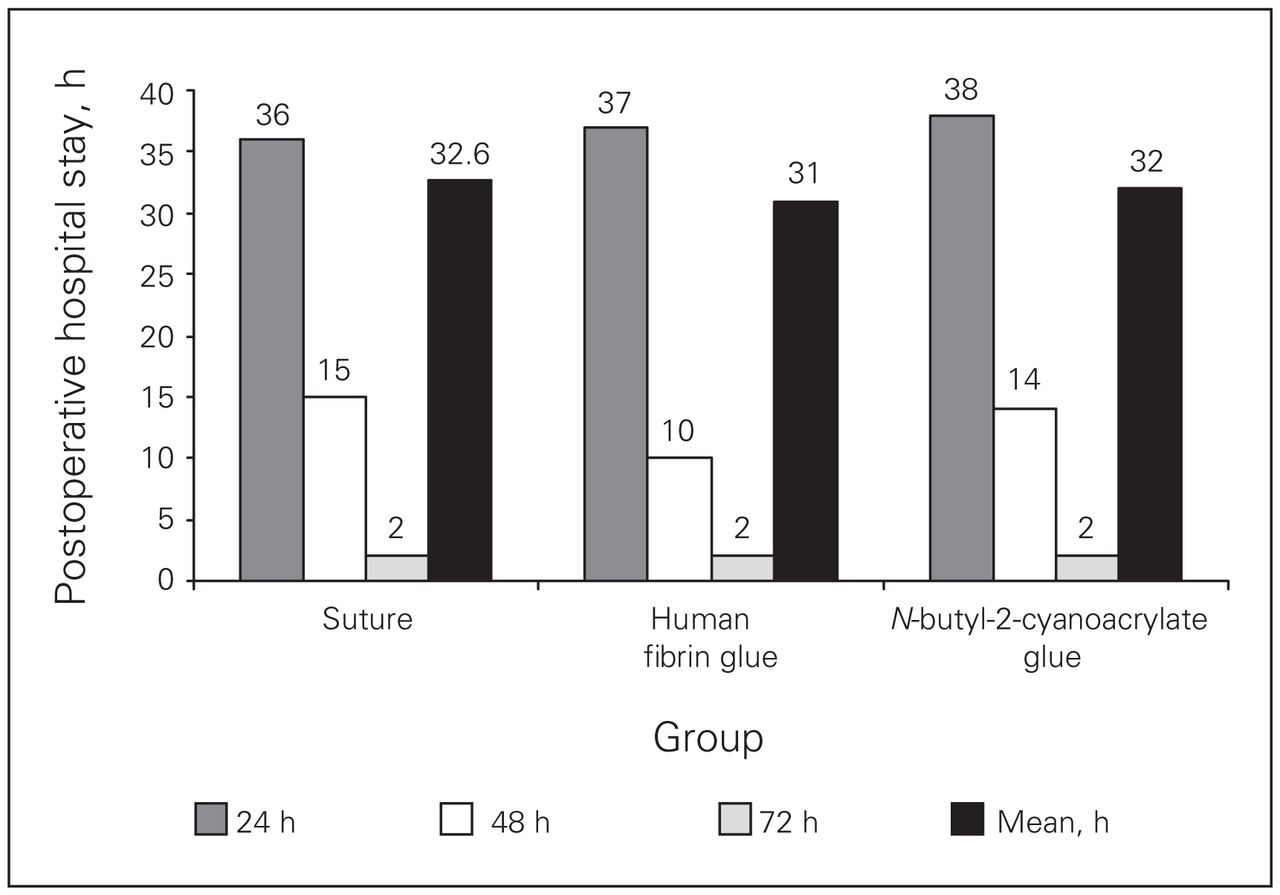
Mean length of postoperative hospital stay among patients who underwent inguinal hernia repair with sutures, human fibrin glue or N-butyl-2-cyanoacrylate.
The mean time to return to work was 20.4 (SD 3.38) days in the suture group, 20.3 (SD 3.94) days in the fibrin glue group and 19.8 (SD 3.63) days in the N-butyl-2-cyanoacrylate group (p = 0.60).
During the long-term follow-up (Table 3), 2 patients (3.39%) reported moderate chronic pain resolved by the use of analgesic therapy at 3 and 6 months in the suture group; no patients in the fibrin glue or N-butyl-2-cyanoacrylate groups reported such pain. Five patients (8.74%) in the suture group reported sensations of an extraneous body; 1 patient (1.78%) reported this in the N-butyl-2-cyanoacrylate group. In total, there were 7 long-term complications (11.86%) in the suture group, 0 long-term complications in the fibrin glue group and 1 long-term complication (1.78%) in the N-butyl-2-cyanoacrylate group (suture v. fibrin glue, p = 0.01; suture v. N-butyl-2-cyanoacrylate, p = 0.03; fibrin glue v. N-butyl-2-cyanoacrylate, p = 0.30). No cases of mesh displacement, plug migration causing complication, or urinary retention were observed. No patients reported severe chronic postherniorrhaphy pain or had more than 1 complication during follow-up.
Long-term outcomes among patients who underwent plug and mesh hernia repair with sutures, human fibrin glue or N-butyl-2-cyanoacrylate
Discussion
Nearly 800 000 patients undergo surgery for inguinal hernia repair in the United States each year, making this disease a major public health issue.27,28 Before the revolution of inguinal hernia repair by tension-free techniques about 20 years ago, traditional groin hernioplasty techniques (i.e., Bassini, Postempsky, McWay, Shouldice) were associated with a high rate of recurrence and a high rate of postoperative chronic pain because of the tension of the tissue.4,29–31 An improvement in postoperative comfort and a lower incidence of recurrence have been reported among patients who undergo tension-free techniques compared with non-mesh techniques.4
However, up to 75.5% of patients report chronic pain during the long-term follow-up after mesh repair,2,6,32–34 and this complication was probably previously underestimated. In a Danish nationwide questionnaire study that included 1652 patients undergoing surgery for inguinal or femoral hernia repair, a high incidence (11%–17%) of chronic pain leading to various types of social disability was documented.5 Perkins and Kehlet35 also reported an overall incidence of 12%.
Because recurrence is rare among patients who receive wall reinforcement with prosthetic mesh (0%–2%)36,37 and because the sensation of a foreign body is not an important limiting factor, chronic pain is now the most important complication associated with hernia mesh repair using the plug and patch technique. In fact, postherniorrhaphy pain can significantly influence the patients’ quality of life. Moreover, some authors report that a significant proportion of the pain is of neuropathic origin.5,33,35,38–41 Because of this, when genitofemoral, ilioinguinal and/or iliohypogastric nerves are damaged by suture entrapment or by contact with mesh, the probability of acute or chronic pain after surgery is very high.
Despite criticism for technical difficulties, cost and a long learning curve,42–44 laparoscopy for extraperitoneal or transabdominal preperitoneal procedures is currently the standard alternative approach to open surgery for hernia repair,45,46 bilateral or recurrent disease and decreasing postoperative pain. However, laparoscopic herniorrhaphy is not without complications related to the use of staples to fix the mesh to prevent its displacement with consequent hernia recurrence, and this approach requires general anesthesia. Sensory nerve entrapment with neuralgia, bleeding and hematomas in the Retzius space, and chronic groin pain have been reported.47–50 The potential complications associated with stapled mesh fixation has led surgeons to consider an alternative method of mesh fixation; many experimental9,49 and clinical22,23,51–57 studies have reported the use of glue for prosthetic mesh fixation during laparoscopic procedures or for suture during open inguinal hernia repair. However, a meta-analysis of randomized controlled trials concluded that persistent pain occurred less frequently after laparoscopic repair than after open mesh placement.57
After the successful use of fibrin glue or N-butyl-2-cyanoacrylate glue in hernia surgery, we decided to perform a prospective, randomized controlled trial to compare the efficacy of human fibrin glue, N-butyl-2-cyanoacrylate and suture during 1-day surgery open inguinal hernia repair. This regimen of admission was used when the study was started in 2003; for this reason, despite the fact that this procedure is now usually performed as day surgery, the study was completed in 1-day-surgery regimen, to preserve the homogeneity of the method.
We found no significant differences in operation time, postoperative length of hospital stay and time to return to work among the 3 groups. However, the overall morbidity rate was significantly lower in both the fibrin glue and N-butyl-2-cyanoacrylate groups than in the suture group. Both short- and long-term outcomes were significantly improved using glues compared with sutures. Moreover, there were no significant differences between the N-butyl-2-cyanoacrylate group and the fibrin glue group. Although inflammatory reaction and retractile fibrosis in the N-butyl-2-cyanoacrylate group might lead to a hypothesis of a higher incidence of the sensation of an extraneous body in the inguinal canal, this was not statistically confirmed in our study by even 1 event. However, this may be an important finding, but further investigation is needed in more patients.
The reasons for the better short- and long-term results with glues than with sutures are probably related to injury from the sutures to the nerves and vessels. In this study, all operations were performed by the same surgeon, keeping potential biases because of interoperator variability to a minimum.
This study demonstrates that fibrin glue and N-butyl-2-cyanoacrylate are better tolerated than sutures by patients, and that the glues lead to better results during initial follow-up and a better trend in long-term data. There did not seem to be differences between the 2 types of glue. In conclusion, we recommend using glues in tension-free inguinal open repair with the plug and mesh technique.
Footnotes
Competing interests: None declared.
Contributors: Drs. Testini, Poli and Piccinni designed the study. Drs. Lissidini, Gurrado and Lardo acquired the data, which Drs. Testini, Poli and Lardo analyzed. Drs. Testini, Poli and Piccinni wrote the article, which Drs. Testini, Lissidini, Gurrado and Lardo reviewed. All authors approved the article’s publication.
- Accepted June 3, 2009.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.